15
Extreme Impactions, Unusual Phenomena and Difficult Decisions
Case 1: Monster tooth, supernumerary tooth, impacted central incisor and the maxillary midline
Case 2: Bilaterally impacted maxillary canines in a patient suffering with aggressive juvenile periodontitis
Case 3: Labially impacted maxillary canine at the level of the nasal floor
Case 4: Impacted mandibular molars and premolars with over-eruption of the opposing teeth
Case 5: Severe trauma in infancy causing damage to anterior tooth buds
Case 6: Buccal to the lateral incisor and palatal to the central incisor
In this chapter, the intention is to present a few cases featuring impacted teeth in a variety of difficult, interdisciplinary or extreme situations. For these cases, there are no hard-and-fast rules, the literature offers the practitioner little assistance and, despite all the advice that may be sought and received, the orthodontist largely remains alone in a diagnostic or treatment planning wilderness without a compass. Options may be few, but they also may be so many that each potential scenario must be acted out in the fertile imagination of the orthodontist to find the direction that will offer relative success, cause the least collateral damage and carry with it the least risk of failure. Some may require the active participation of specialists in fields other than orthodontics and oral surgery, particularly the paediatric dentist, the endodontist and the periodontist. By their very nature, these cases are frequently one of a kind and thus determining the diagnosis, the treatment options, chosen treatment approach and prognosis may never be evidence-based, but largely dependent on the logic acquired from the collected clinical experience of the operators.
This is both the strength and the weakness of published single case reports. There is often much to learn from them individually but, whatever that may be, it cannot be used to draw conclusions in relation to other apparently or arguably similar cases in the future. Without doubt legitimate criticism may be levelled by any dentist regarding the treatment decisions that were made in the following individual presentations. Moreover, an alternative approach to the same case might be preferred, a choice that will be influenced or biased by that orthodontist’s positive or negative experience with the same or contrary modalities of treatment.
The clinical cases shown here are mostly finished cases with long-term post-treatment follow-up and they are offered here specifically as they relate to impacted teeth. Others are in the final stages of their overall active treatment as this book goes to print but, in all cases, the principal issue under discussion (i.e. resolution of the impaction) will have been fully and successfully addressed.
Case 1: Monster Tooth, Supernumerary Tooth, Impacted Central Incisor and the Maxillary Midline
The existence of an unusually large maxillary central incisor with talon cusp or cusps, otherwise known as dens evaginatus, is rare and usually published in the literature as a single case report [1–3]. Since it takes up more than the space of a normal central incisor and its location is at the front of the mouth, the dens evaginatus is unsightly and disfiguring. To reduce it in size with the view to reshaping it to more normal proportions is difficult or impossible, because of a large pulp chamber and/or a very broad cross-section in the cervical region. In such circumstances, it is often extracted and replaced prosthetically, or it may be enlarged and reshaped to make it resemble two teeth, a central and lateral incisor, while sacrificing the adjacent normal and healthy lateral incisor.
In the present case of a 7-year-old healthy girl (Figure15.1a-e), the right central incisor was much enlarged with a Y-shaped crown cross-section, due to the talon cusp and a much enlarged pulp chamber and root cross-section at the CEJ. The dentition comprised the four erupted first molars, mandibular central incisors and rotated erupting mandibular lateral incisors, associated with mild dental crowding. On the maxillary left side, there was an atypical incisiform ‘central incisor’, which was assumed to be a supernumerary tooth. The dens evaginatus occupied most of the space for both central and lateral incisor of that side. The remainder of the dentition comprised healthy and restored deciduous teeth in normal intermaxillary occlusal relations.
Periapical and panoramic radiographs (Figure 15.1f, g) revealed the unerupted teeth superimposed on one another with inadequate differentiation for appropriate diagnosis. Accordingly a CBCT was performed (Figure 15.1h, i) from which it was concluded that the unerupted teeth in the maxillary incisor region included two normal lateral incisors and an unerupted, normally shaped, left maxillary central incisor. This lent credence to the assertion that the erupted ‘central incisor’ was a supernumerary tooth and that the dens evaginatus represented a fusion between a right central incisor and an additional supernumerary tooth.
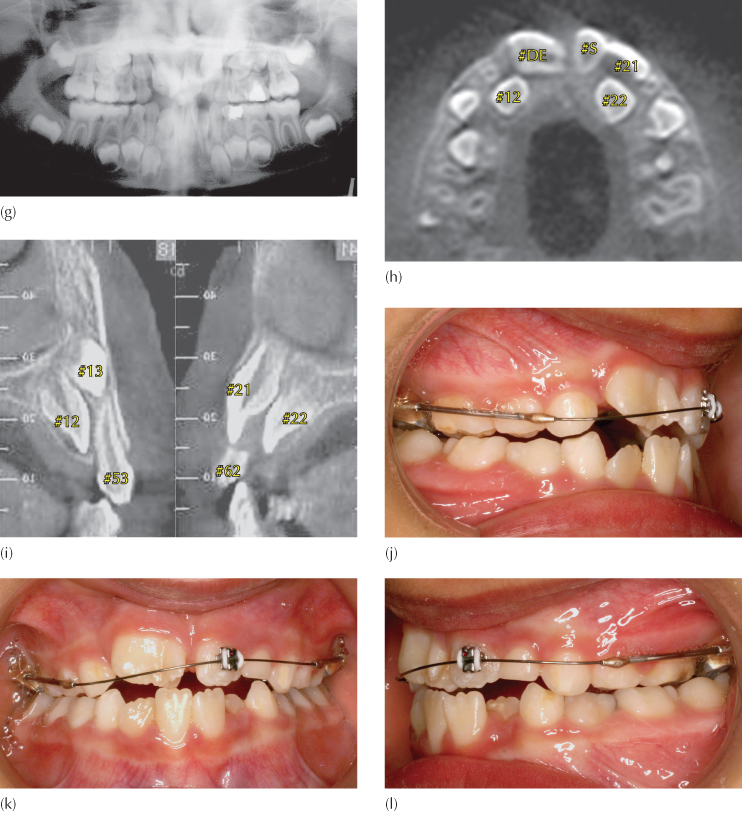
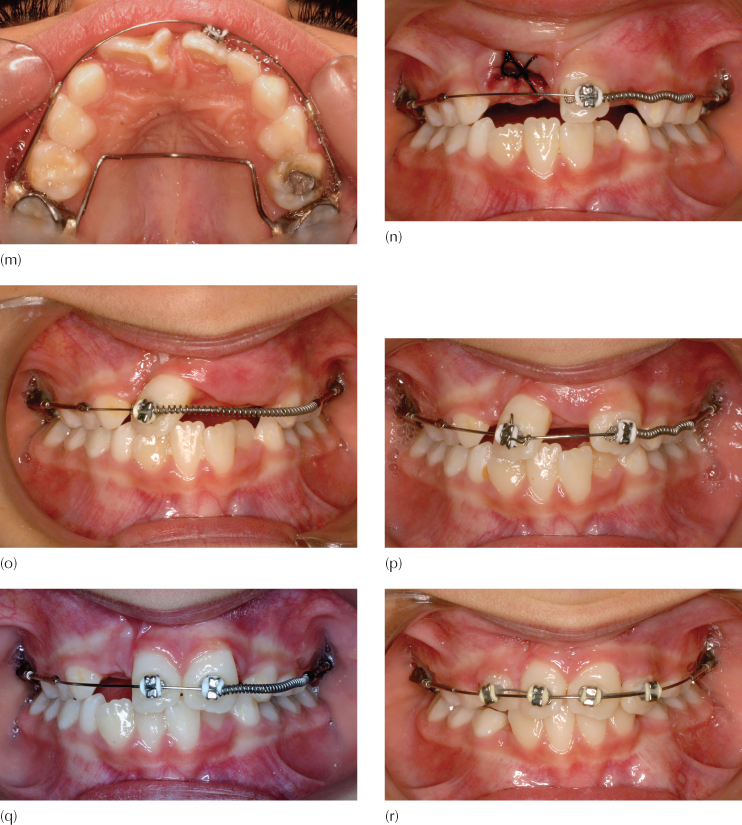
Fig. 15.1 (a–e) The clinical intra-oral views. (f, g) Periapical and panoramic radiographic views. (h) CBCT axial cut through the roots of the erupted teeth. #D.E is the dens evaginatus and #S the erupted supernumerary tooth. (i) Right and left CBCT transaxial views. (j-m) The modified Johnson 2 × 4 (2 × 1) appliance in place. (n) Following the extraction of the dens evaginatus, a coil spring is compressed between the soldered stop on the mesial end of the left buccal tube arm and the bracket on the supernumerary tooth. (o) With the TipEdge bracket, tipping of the left supernumerary across the facial midline takes only six weeks. (p) Four months later, the left central incisor has erupted and is incorporated in the appliance, with a coil spring moving it to the midline, while the supernumerary tooth is being uprighted in the right central incisor position. (q) The condition prior to lateral incisor eruption. (r) The lateral incisors erupt spontaneously and are incorporated in the appliance. (s–u) The completion of phase 1 treatment. (v, w) Panoramic and periapical views clearly show the midline suture on the right side of the supernumerary tooth, together with an enlarged right canine dental follicle/early dentigerous cyst. (x) The midline raphe is seen to deviate sharply to the right in this pre-phase 2 occlusal view of the palate, as indicated by the arrows. The incisive papilla has also been displaced. The dental follicle of the unerupted right canine has enlarged into a small dentigerous cyst and can be seen to have expanded the alveolar ridge. (y) The pre-phase 2 view of the patient from the front shows a pleasing appearance, a normal dental smile line and an apparently natural dental midline.
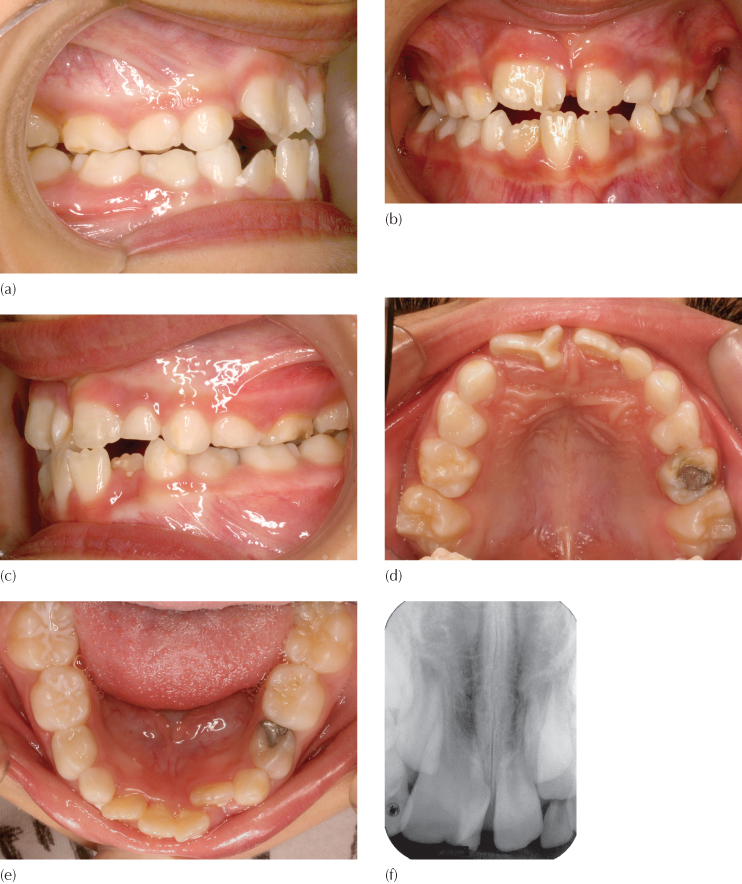
The shape and size of the dens evaginatus, together with its pulp chamber dimension and cross-sectional breadth at the CEJ, determined that the limited alteration of crown shape possible would not provide a satisfactory answer to the overall space problem, nor would it contribute to improving the patient’s appearance. Thus, its extraction was unavoidable. This created the unbalanced situation in which an incisor would be missing on the right side, while an extra incisor was present on the other.
The treatment proposed, therefore, was to move the erupted and presumed supernumerary tooth across from the left to fill the place of the extracted dens evaginatus on the right side and thus to permit the eruption of the impacted normal left central incisor tooth into its designated place. Once this was completed, the deciduous canines in both jaws would be extracted to provide space temporarily to permit the alignment of the four incisors in both jaws.
A modified form of the 2 × 4 appliance (in fact, a 2 × 1 appliance) was placed, with a palatal arch soldered to two molar bands and the typical modified Johnson twin arch set-up described in Chapter 5, with a Tip-Edge® bracket placed on the single erupted permanent supernumerary incisor and an archwire of 0.016 in round steel wire inserted into the buccal arms of the composite archwire which, in turn, would be inserted into the molar tubes (Figure 15.1j–m). The orientation of the soldered molar tubes and these buccal arms was tipped slightly downwards on each side to encourage incisor eruption and bite closure and a welded stop was placed on the buccal arms of each side mesial to the molar tubes to maintain the initial arch length and to prevent unwanted sliding of the buccal arms through the tubes.
The abnormal right dens evaginus central incisor was extracted at the next visit and, on the same day, a coil spring was compressed between the soldered stop at the mesial end of the left buccal arm and the bracket on the left erupted incisiform supernumerary tooth (Figure 15.1n). Six weeks later, the tooth was seen to have tipped across the midline and into proximal contact with the deciduous canine of the opposite side (Figure 15.1o). The impacted left central incisor erupted rapidly and autonomously five months after placement of the coil spring, driven by the sudden provision of space in the arch. This tooth was bracketed and a coil spring again placed on the arch to move it to the midline. An auxiliary spring was placed in the vertical slot of the Tip-Edge® bracket of the supernumerary tooth to upright its root across the facial midline (Figure 15.1p, q).
During the subsequent 12 months of treatment, the four deciduous canines were extracted and the lateral incisors erupted without further assistance. Brackets were placed on them and the teeth were aligned and moved towards and slightly across the midline. Further root uprighting was then initiated (Figure 15.1r). Phase 1 treatment was completed seven months later, with satisfactory alignment of the teeth (Figure 15.1s-u). The root configuration of the substitute ‘right central incisor’, formerly the supernumerary tooth (Figure 15.1v, w), strengthens the assumption that it was indeed a supernumerary tooth.
It should be clearly understood that moving a tooth across the left side of the maxilla to the right, across the midline, does not infer that the tooth actually traverses the midline palatal suture. What happens is that the bone on each side of the suture is remodelled and moves together with the tooth, so that the suture remains on the mesial side of the left incisor, as can be seen on the radiographs and the radiograph (Figure 15.1v–x).
The total treatment time was 26 months, a removable maxillary Hawley retainer is being worn nightly and phase 2 treatment will be considered in the full permanent dentition.
Case 2: Bilaterally Impacted Maxillary Canines in a Patient Suffering with Aggressive Juvenile Periodontitis
The patient was a 15-year-old girl, who had been referred to the author for the treatment of her bilaterally impacted maxillary canine teeth. No mention was made in the referral letter to the effect that the patient suffered from periodontal disease and there were no symptoms that might have indicated this.
An examination of the initial panoramic view (Figure 15.2a) indicated a routine palatal impaction of both maxillary canines, both classified as group 1 type (see Chapter 6). Clinically, there was a close to normal occlusion with excellent alignment in both jaws, good intercuspation and a normal overbite and overjet.
(a) Initial panoramic view with bilateral maxillary palatal canine impaction. The typical picture of aggressive juvenile periodontitis is seen, with deep vertical periodontal defects and severe bone loss in the four molar and maxillary incisor regions.
(b) A new panoramic film taken after the successful completion of periodontal treatment shows the radio-opaque areas where bovine bone was used to regenerate bone in the defective areas. (Periodontics by Professor Ayala Stabholz.)
(c–e) The post-periodontic intra-oral appearance of the malocclusion.
(f–h) After extraction of the maxillary deciduous canine, orthodontic alignment, levelling and space opening, the canine spaces are held open with the use of cut lengths of stainless steel tube of broad gauge (0.036 in internal diameter) threaded onto the main arch.
(i–k) At surgery, the orthodontist has bonded an eyelet attachment to the exposed canine and traction is applied using an elastic chain stretched between the inverted power pins on the adjacent teeth. This is raised in its middle portion to engage the twisted pigtail ligature that has been turned into a small hook close to the sutured tissues.
(Surgery by Dr H.P. Samen.)
(l–n) At 8 years following the completion of orthodontic treatment, there is an excellent alignment and appearance of the gingival tissue around the previously impacted canines. There are no signs that these had been impacted.
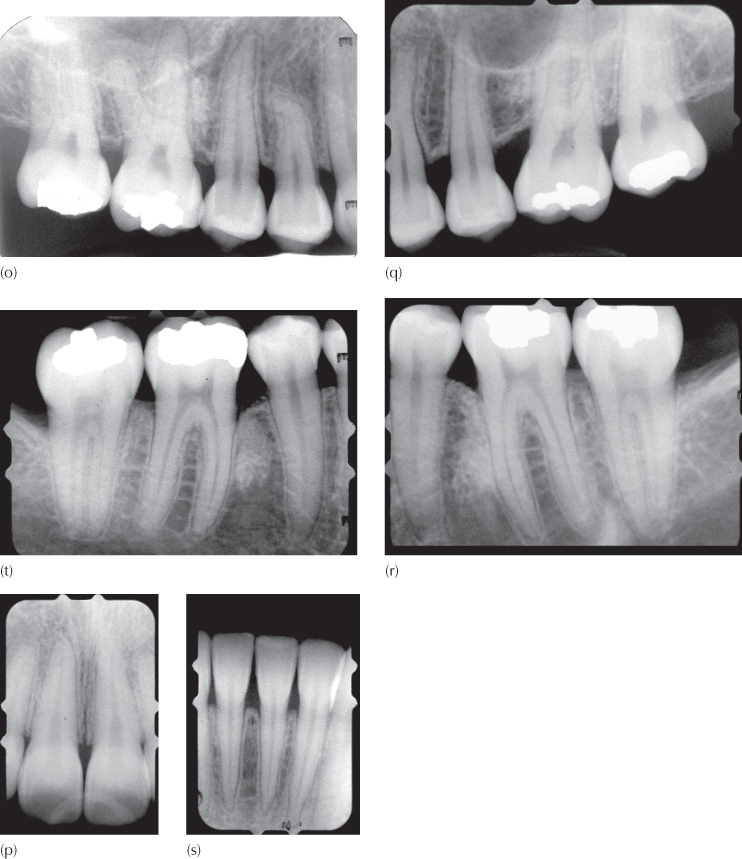
(o–t) Periapical views of the areas that were most seriously affected by the condition, seen eight years post-treatment.
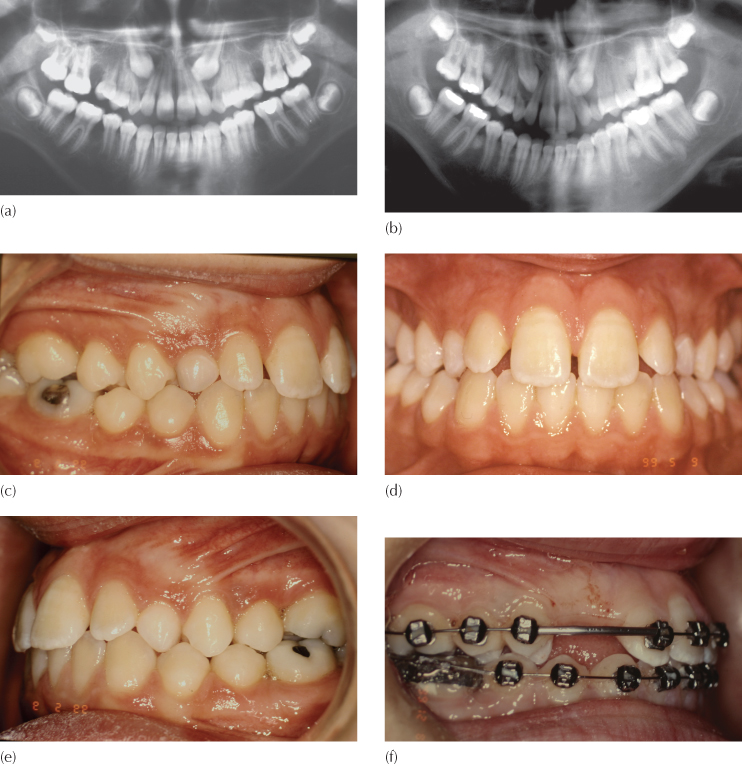
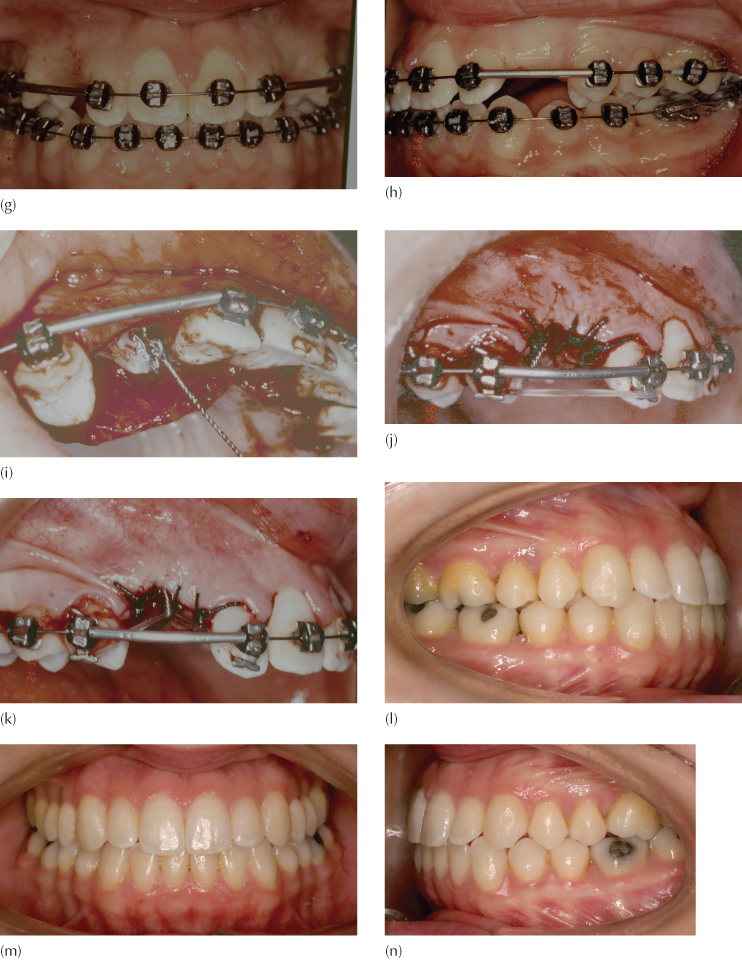
The complicating factor here was that the patient suffered from aggressive juvenile periodontitis, with the loss of much alveolar bone in the molar and incisor regions of both jaws. The patient returned 18 months later having completed her periodontal treatment, which included the grafting and integration of bovine bone in the more severely affected locations mesial to the first molars (periodontic treatment by Professor Ayala Stabholz). These may be clearly seen as small radio-opacities on the new film after a long period of post-treatment follow-up (Figure 15.2b). Note also the spontaneous closure of the spaces between the second premolars and the first molars which had been present before treatment began.
Pre-surgical orthodontic preparation for this almost normal occlusion (Figure 15.2c–e) involved levelling, aligning and space-opening and lasted just four months, before closed exposures were performed on both canines (Figure 15.2f–h). A measured length of steel tube was threaded over the base arch, with the purpose of holding the distance between the premolar and lateral incisor brackets. The right side is shown here, to illustrate the use of an elastic e-link stretched between the occlusally inserted power pins into the vertical slots of the Tip-Edge® brackets of the lateral incisor and first premolar, which was then raised and engaged in the pigtail ligature close to the sutured flap. In this way, renewable vertical traction was applied to the impacted teeth to bring about their eruption (Figure 15.2i–k). The final result, shown here eight years after completion of the orthodontic treatment (Figure 15.2l–n), shows excellent alignment and inter-arch relations. The clinical appearance of the teeth and the new periapical radiographs offered no signs or clues that would indicate that the canines had previously been palatally impacted (Figure 15.2o–t). While still discernible in the radiographs, the bone grafts have become progressively more integrated into the trabecular picture. The orthodontic treatment time for this case was 18 months and the patient is followed up by the periodontist on a regular basis.
Case 3: Labially Impacted Maxillary Canine at the Level of the Nasal Floor
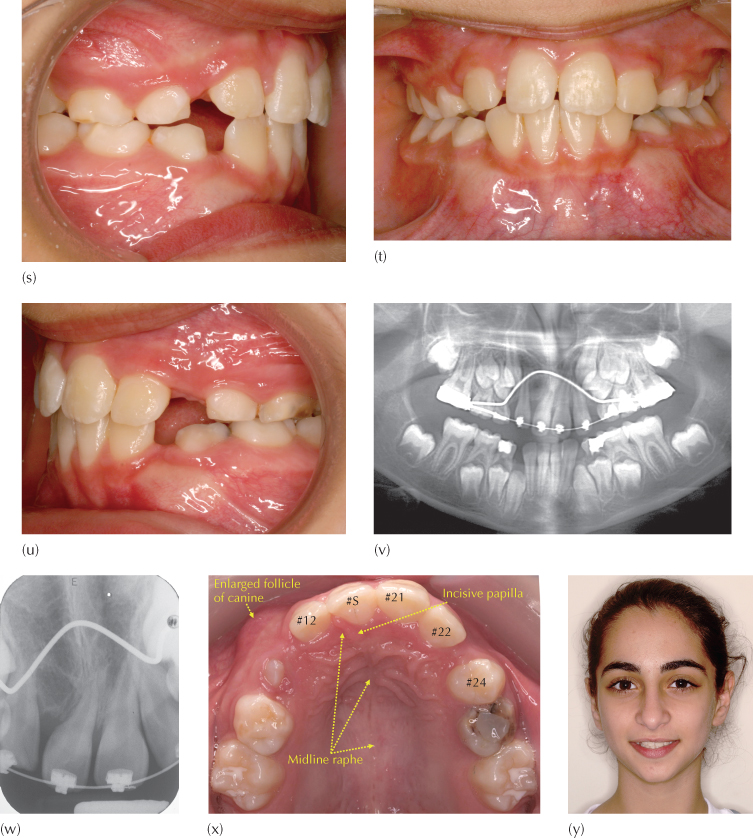
The patient, a girl aged 11 years in the late mixed dentition stage, was referred to the author with accompanying radiographs from which bilateral labially impacted upper canines had been diagnosed, one of which was extremely high in the maxilla.
The existing occlusion was almost ideal, with good general dental alignment, a class 1 occlusal relationship of the molars and normal incisor overbite and overjet (Figure 15.3a-c). The panoramic radiograph (Figure 15.3d) showed the presence of a lingual arch space maintainer, which had been placed following the extraction of deciduous teeth. It showed the presence of all the permanent teeth, together with the about-to-be-shed maxillary left first and second deciduous molars and the mandibular left second deciduous molar. The two maxillary deciduous canines were also present with virtually complete and unresorbed roots. The maxillary left first premolar root w/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


