Dental Cement
Chapter Objectives
Upon completion of this chapter, the student will be able to:
2. Discuss the uses of cements in dentistry for:
• Luting
4. Discuss the components of each dental cement.
5. Discuss how these components affect the properties of the cement.
6. Discuss the advantages and disadvantages of each cement.
7. Discuss the manipulation considerations for mixing cements.
8. Describe the procedure for filling a crown with luting cement.
9. Describe the procedure for removing excess cement after cementation.
KEY TERMS defined within the chapter
Low-Strength Base/Liner a thin layer of material placed to protect the tooth from the components of dental materials and microleakage, to stimulate reparative dentin, or to act as a pulp capping
Secondary Consistency thick, putty-like, condensable material that can be rolled into a ball or rope, suitable for use as a base
High-Strength Base/Liner a thick layer of cement used to protect the tooth from chemical and thermal irritation
Permanent lasting indefinitely
Primary Consistency less viscous, flows easily, can be drawn to 1-inch string with a spatula lifted from the center of the mass, suitable for luting
Temporary/Provisional materials expected to last from a few days to a few weeks
Intermediate materials expected to last from a few weeks to a year
Sedative to soothe or act in a sedative manner, to relieve pain
Adhesion the bonding of dissimilar materials by the attractive forces of atoms or molecules
Few materials in dentistry are used as frequently or with as much variation as dental cements. Many dental cements are available, and each may have specific or multiple uses. No single cement is universally acceptable and fulfills all applications; rather a variety of cements are available whose properties and manipulation lead them to be an appropriate choice for a given application. In most cases, cements have inferior strength and high solubility when compared with other restorative materials and, with the exception of resin and glass ionomer cements, have little or no adhesive properties. However, the use of cements in a wide variety of dental procedures is extensive. With the multitude of available cements and their applications, it is easy to become confused as to which cement should be selected for a given situation. In most cases, the dentist will select the cement for the procedure on the basis of mechanical as well as biological considerations. It becomes the dental assistant’s responsibility to manipulate the cement to the proper consistency within a specific time frame. Many expanded function auxiliaries may also be placing the cement and removing it at the end of a procedure. The dental hygienist may be placing and removing cements and instrumenting against their surface during periodontal procedures. It is important that the allied oral health practitioner have a thorough understanding of cement uses, properties, limitations, and manipulation to effectively utilize these materials.
Uses of Dental Cements
Pulpal Protection
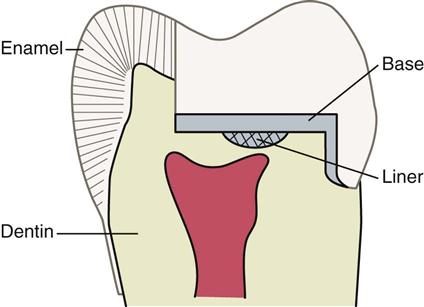
The bacterial effects of caries, the biological response to chemicals contained in restorative materials, and even the cutting of tooth structure may cause pulpal irritation. Pulpal irritation can also occur as the result of thermal conductivity of metal restorations placed near the pulp, and when the dentin remaining over the pulp is too thin to withstand compressive, tensile, and shearing stresses. Cavity varnishes, liners, and bases act as protective layers between the dentin and the restorative material (Figure 13-1).
Cavity Varnish
Cavity varnish acts as a protective barrier between preparation and restoration. Varnish formulations are solutions of natural resins (copal) or synthetic resins dissolved in a solvent such as alcohol or chloroform. The varnish is applied in two to three layers over the surface of the preparation. The solution is placed in a thin film, allowing evaporation of the solvent to occur for 5 to 15 seconds before application of the second layer. The remaining resin protects the pulp by sealing the tubules from the penetration of irritating chemicals found in some restorative materials and luting agents. This resin varnish also reduces the amount of microleakage and staining at the restoration/tooth interface. The varnish is supplied in two bottles; the primary bottle is 90% solvent and 10% resin. A separate bottle of solvent is supplied to dilute the material in the primary bottle when it thickens as the solvent evaporates. The lid of the varnish must be kept tightly capped to avoid evaporation of the solvent. Copal varnishes, although popular for many years, are not used much any longer because they wash out within a few months. Today’s dentin bonding agents, which also seal enamel and dentinal tubules, have largely replaced the use of varnish.
Low-Strength Base/Liner
Calcium hydroxide is used as a low-strength base/liner in cavity preparations in which dentin no longer covers the pulp. When very small exposures of the pulp are suspected, this material is used as a direct pulp-capping agent. The two-paste system is composed of calcium hydroxide, zinc oxide, and glycol salicylate. Equal amounts of catalyst and base pastes are incorporated to a creamy consistency.
Calcium hydroxide has an alkaline pH of between 9 and 11. This alkali stimulates secondary dentin when in direct contact with the pulp, providing a barrier between pulp and restoration. It has some thermal insulating properties and provides minimal strength to support the forces of condensation. Questions about the long-term success and retention of these bases and the development of dentin bonding systems have greatly reduced the routine use of this material.
High-Strength Base/Liner
Bases provide thermal insulation and support for restorations. Cements used as bases are mixed to secondary consistency—a thick putty-like consistency that is condensable and can be rolled into a ball or rope. Bases placed in a thickness of 0.5 mm or greater provide protection from the thermal conduction of metallic restorations. When the cavity preparation is so deep that there is 2 mm or less of remaining dentin over the pulp, many clinicians will choose to provide mechanical support for the restoration by first placing a cement base.
Buildup
A buildup, much like a high-strength base/liner, provides mechanical support for a restorative material when an excessive amount of tooth structure is removed. The remaining tooth structure may first need to be rebuilt to better support the restorative material or to act as a foundation before crown preparation. With placement of a cement buildup, the compromised tooth is reinforced.
Luting-Cementation
Successful cementation ensures predictable retention for the indirect restoration. The restorative material itself may be the primary determinant for the cement selection. When choosing a luting agent, the clinician must consider which of the following indirect restorations are being utilized:
• Metal and metal-based restorations—crowns, bridges, inlays, or onlays
Other considerations include whether the preparation has some mechanical retention and the patient’s parafunctional habits.
A luting agent is a viscous material placed between tooth structure and a prosthesis that sets and firmly attaches the prosthesis to the tooth structure. New luting agents with adhesive capability are being introduced in an attempt to improve the clinical success of fixed prosthodontics.
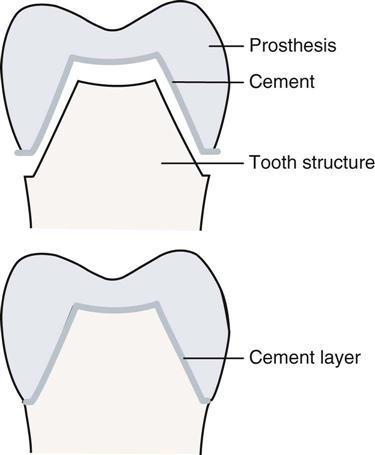
Cements used for permanent or temporary luting, that is, cementing of two components together, of fixed prostheses, orthodontic bands and brackets, and pins and posts must have good wettability and flow to provide a thin film thickness. When the tooth structure and the fixed prostheses are in intimate contact, a microscopic space exists—the tooth/restoration interface. The primary purpose of luting cement is to fill this space (Figure 13-2). Cements mixed to primary consistency must have thin enough viscosity to be able to flow into a film thickness of .25 µm or less. If the viscosity of the cement is such that the prosthesis fails to regain intimate contact with the tooth, a thick layer of cement will be exposed at the margin. This may also occur if the margins do not fit precisely before luting. Exposure of cement to oral fluids at the margins results in dissolution of the cement. As cement is lost at the margins, bacterial plaque can accumulate beneath the crown where the patient cannot clean, resulting in recurrent caries. Some cements have the capability of chemically bonding the prosthesis to the tooth. The chemical bond enhances retention by reducing separation of the tooth/prosthesis interface.
Orthodontic Bands and Brackets
Orthodontic bands and brackets are retained on teeth for several months or even years. Brackets are usually bonded directly to the tooth structure (see Chapter 5), while bands are luted with a dental cement. The cement must adhere tenaciously to the enamel and the orthodontic appliance to provide leverage for tooth movement. Demineralization of the tooth surface due to solubility of cements and resultant leakage of bacteria between the bands and the tooth surface has been problematic for many patients. This concern has been minimized to some extent with fluoride-releasing cements.
Restorations
Permanent, Temporary, and Intermediate
Because of their lower strength and wear resistance and higher solubility, cements are not frequently chosen as permanent restorations. The exception is glass ionomer cement, which, because of its release of fluoride, is utilized for class V restorations of root caries in adults and for restoration of primary teeth. (See Chapter 6.)
As provisional and intermediate restorations, dental cements are mixed to secondary consistency. The choice of cement for this type of restoration is largely based on the particular clinical situation. Provisional restorations are used for emergency situations when appointment scheduling does not allow sufficient time to place a permanent restoration. Provisional restorations are placed when a tooth is symptomatic or when deep caries removal is required. By placing a sedative provisional restoration, the dentist is able to evaluate the response of the pulp before reappointment for a permanent restoration. Provisional and intermediate restorations are used to restore teeth awaiting treatment such as inlays, between endodontic appointments, or when extensive treatment plans require several weeks or months of coverage before treatment can be completed.
See Chapter 14, Provisional Restorations, for a discussion of intracoronal cement provisionals.
Surgical Dressings
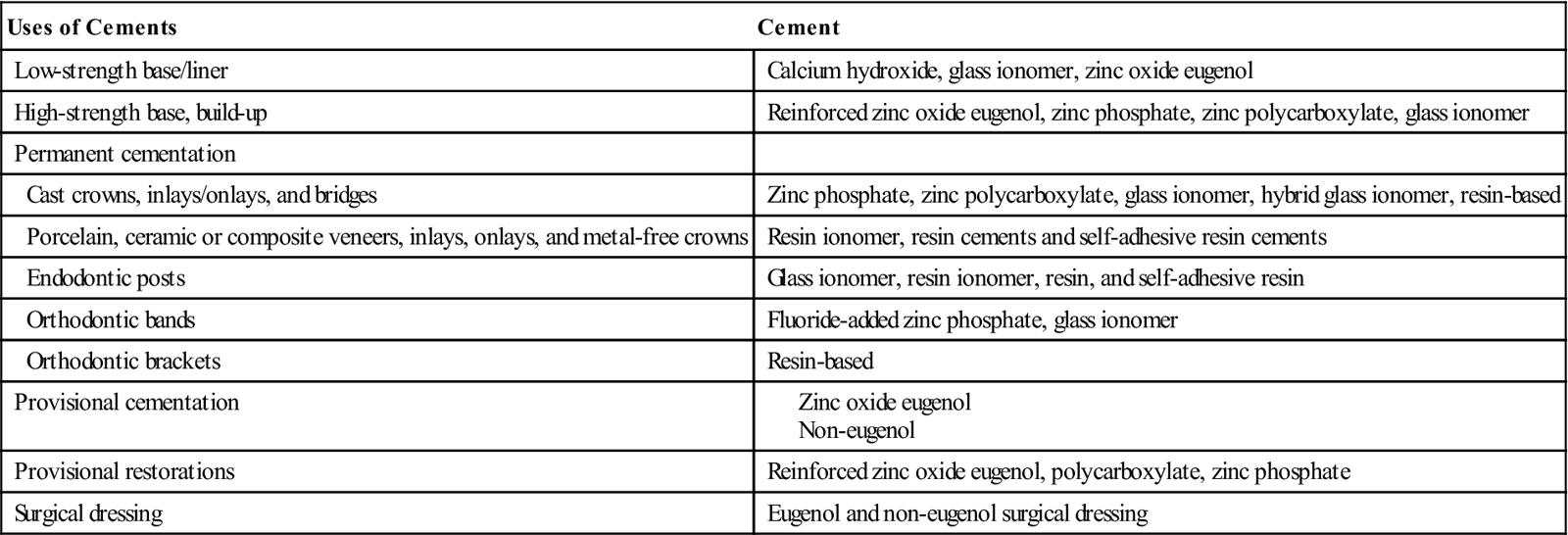
As a surgical dressing, cements are used to provide protection and support for the surgical site, to provide patient comfort, and to help in the control of bleeding. Most clinicians prefer a non-eugenol dressing, which may be dispensed in both light-cure and chemical-cure formulas. These materials are mixed to a soft putty-like consistency; they harden when placed over the tissue, forming a rigid covering (Figures 13-3 and 13-4) (Table 13-1).
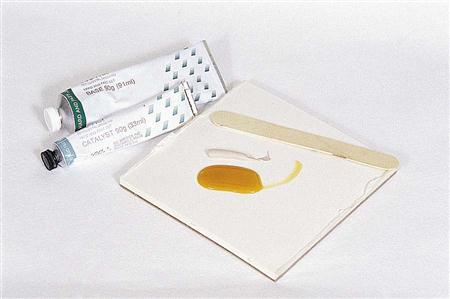

TABLE 13-1
< ?comst?>
< ?comen?>< ?comst1?>
< ?comst1?>
< ?comen1?>
Properties of Dental Cements
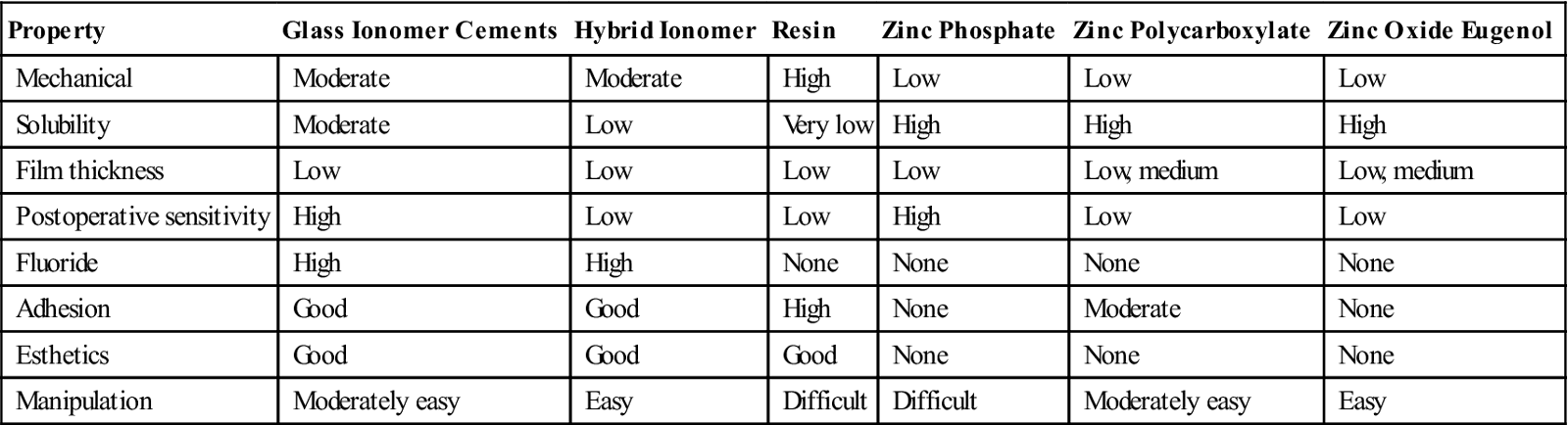
Properties of dental cements differ from one type of cement to another. No cement is ideal for every clinical situation. Although one type of cement may be appropriate for a single crown, it may not be ideal for a multiple-unit bridge; some cements work well on metal surfaces, but others are more appropriate for ceramic or porcelain surfaces. The clinician must consider both physical and biological properties when selecting cement for a specific dental procedure. The most important properties are strength, solubility, viscosity, biocompatibility, retention, esthetics, and ease of manipulation (Table 13-2).
TABLE 13-2
< ?comst?>
| Property | Glass Ionomer Cements | Hybrid Ionomer | Resin | Zinc Phosphate | Zinc Polycarboxylate | Zinc Oxide Eugenol |
| Mechanical | Moderate | Moderate | High | Low | Low | Low |
| Solubility | Moderate | Low | Very low | High | High | High |
| Film thickness | Low | Low | Low | Low | Low, medium | Low, medium |
| Postoperative sensitivity | High | Low | Low | High | Low | Low |
| Fluoride | High | High | None | None | None | None |
| Adhesion | Good | Good | High | None | Moderate | None |
| Esthetics | Good | Good | Good | None | None | None |
| Manipulation | Moderately easy | Easy | Difficult | Difficult | Moderately easy | Easy |
< ?comen?>< ?comst1?>
< ?comst1?>
< ?comen1?>
Strength
Cements are brittle materials with good compressive but more limited tensile strength. The strongest cements are resin cements, and the weakest is zinc oxide eugenol. Cements used for permanent luting and high-strength bases need good compressive and tensile strength. As can be seen in Table 13-2, resin-based cement is high in mechanical strength and fracture toughness, and polycarboxylate cement is low in both. Most cements consist of a combination of powder and liquid; their ratio determines many of their properties. The strength of cement is controlled primarily by the amount of powder used in the prepared mix. In general, an increase in the powder-to-liquid ratio increases the strength of the cement. However, excessive powder or liquid can weaken the cement.
Solubility
The tendency of cements to dissolve in the oral fluids, leading to microleakage, recurrent caries, and failure of the restoration, is one of the biggest hurtles for dental cements. Most of the cements used in dentistry will disintegrate in the oral environment over time. Solubility is important whenever the cement is expected to remain exposed to mouth fluids for prolonged periods. Resin-containing cements are as close as possible to being insoluble. Again, the amount of powder incorporated into the final product will influence greatly the solubility of the resultant cement.
Viscosity/Film Thickness
The consistency of mixed cement is the measure of its ability to flow under pressure. This is particularly important in the case of cement used for luting, because it determines the dentist’s ability to seat the indirect restoration properly. For primary consistency, cements should be able to be mixed thin—to about the consistency of honey. Low film thickness is critical to seating and retaining indirect restorations. For a cement to be an effective luting cement, American Dental Association (ADA) specifications require the cement to be able to flow into a film thickness of 25 µm or less.
Secondary consistency requires the addition of powder to increase strength and bring the cement to a thick, putty-like consistency. Cements mixed to secondary consistency are utilized as bases and restorations, temporary or permanent. The addition of powder increases the viscosity and strength and decreases the solubility of the cement.
Several factors influence the consistency of mixed cement. Temperature has a great effect; a lower temperature will slow the setting reaction, giving the clinician more working time and allowing incorporation of more powder into the liquid. Although the amount of powder incorporated into the mix has a direct relationship to strength and solubility, it may substantially increase the viscosity of the mixed cement.
Biocompatibility
Many cements represent a combination of a powder of zinc oxide or powdered glass and an acid. The pH of the acid both at placement and after complete setting is a matter of concern. Postoperative pulpal sensitivity is related to the pH and manipulation variables of the cement. Other causes include unsealed dentinal tubules, trauma to the pulp during preparation, and bacterial leakage under the provisional restoration. Careful attention to powder-to-liquid ratios, dispensing technique, and mixing recommendations can minimize this concern. Eugenol found in the liquid of zinc oxide eugenol cements has an obtundant, sedative effect on the pulp. Fluoride released from powdered glass formulations has an additional property of reducing secondary caries.
Retention
Good adhesion is a critical component of both fixed prosthodonic and restorative dentistry. Adhesion is the bonding of dissimilar materials by the attractive forces of atoms or molecules. Mechanical adhesion is based on the interlocking of one material with another; an excellent example is Velcro. Chemical adhesion is adhesion that occurs at the molecular level when atoms of the two materials swap atoms (ionic bonding) or share outer electrons (covalent bonding). In many dental applications, chemical adhesion and mechanical adhesion occur together. Several things may weaken the strength of the adhesion between two materials, including differences in the coefficient of thermal expansion of the two materials, dimensional changes during setting of the adhesive agent, and contamination of the substrates by water and saliva or by residual enamel and dentin debris, known as the “smear layer.” Failure of the adhesive will result in failure of the indirect restoration due to prosthesis breaking away from the tooth structure altogether, or due to leakage occurring between the tooth structure and the prosthesis, resulting in deterioration of the margins and the formation of secondary caries.
Esthetics
Cements are available in a variety of shades and opacities for luting porcelain veneers, ceramic or composite inlays and onlays, and porcelain full crowns. Usually, a shade is chosen to approximate the shade of the restoration, so that the appearance of the restoration is not altered by the underlying cement as light passes through the restoration and reflects off the cement. Occasionally, it is necessary to mask the color of the dentin, especially if it is discolored. In this situation, an opaque cement of the appropriate shade is selected. Try-in paste is provided by many manufacturers; this water-soluble paste is matched to the base shade of the cement and is used to tack the restoration in place to check the shade of the final product. Try-in paste is recommended to ensure accurate prediction of the final appearance of the restoration and acceptance of restoration esthetics by both the dentist and the patient.
Manipulation
Mixing
It is important that cements be mixed to their appropriate consistency in accordance with manufacturers’ recommendations, with measurement of ratios and meticulous attention to detail. Cements that are mishandled may lead to difficulties in seating or retaining the restoration or pulpal sensitivity. Cements may be hand-mixed or may come in pre-dosed capsules and syringes. Some cements have been packaged in automixing cartridges similar to those used for impression materials (Figure 13-5). Advantages and disadvantages of each delivery system are listed in Table 13-3.

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


