Tomography and panoramic radiography
Introduction
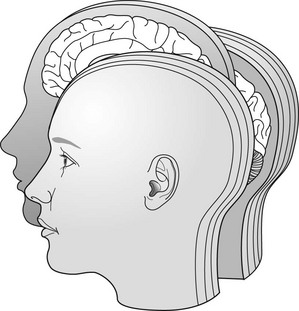
Conventional tomography is a specialized radiographic technique developed originally for producing radiographs that showed only a section or slice of a patient. A useful analogy is to regard the technique as one that enables the patient to be imaged in slices – like a loaf of sliced bread (see Fig. 12.1). Each individual tomographic image (or slice) shows the tissues within that section sharply defined and in focus. The section is thus referred to as the focal plane or focal trough. Tissues and structures outside the tomographic section are not visible because they are very blurred and out of focus.
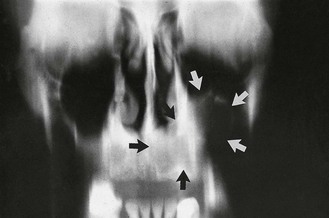
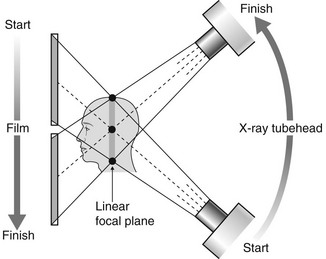
Production of each conventional tomographic slice required controlled, accurate movement of both the X-ray tubehead and the film during the exposure, thereby making it different from all the routine radiographic techniques described in previous chapters. As will be described later in this chapter, by varying the size of the X-ray beam and the type of equipment movement employed it proved possible to change the shape of the tomographic layer from a straight (linear) line (see Fig. 12.2) to a curve, and ultimately to the approximate horseshoe shape of the dental arch, providing an overall panoramic image of all the teeth and their supporting structures – the so-called dental panoramic tomograph (DPT) or panoramic radiograph (see Fig. 12.3).

While panoramic tomography remains very popular, conventional linear tomography has essentially been superseded in radiography by computed tomography, which enables computer-generated tomographic sectional images to be created. Cone beam computed tomography (CBCT) is described in Chapter 13.
Tomographic theory
• Linear tomography using a wide or broad X-ray beam
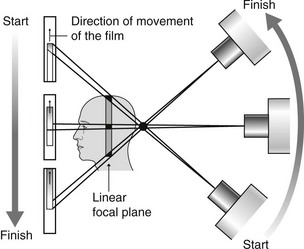
• Linear tomography using a narrow or slit X-ray beam
• Rotational curved tomography using a narrow slit X-ray beam.
Principle of tomographic movement
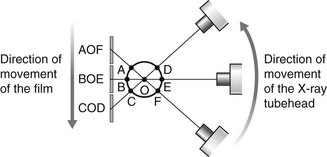
As stated, tomography requires controlled, accurate movement of both the X-ray tubehead and the film. They are therefore linked together. During the exposure, the X-ray tubehead moves in one direction while the film moves in the opposite direction, as shown in Fig. 12.4. The point at the centre of this rotating movement will appear in focus on the resultant radiograph, since its shadow will appear in the same place on the film throughout the exposure. All other points will appear blurred or out of focus.
Broad-beam linear tomography
The principle of tomography illustrated in Fig. 12.4 shows a very thin X-ray beam producing one point (O) – the centre of rotation – in focus on the film. To produce a section or slice of the patient in focus, a broad X-ray beam is used. For each part of the beam, there is a separate centre of rotation, all of which lie in the same focal plane. The resultant tomography will therefore show all these points sharply defined. The principle of broad-beam tomography is illustrated in Fig. 12.5.
Slit or narrow-beam linear tomography
• The X-ray beam has to be collimated from a broad beam to a narrow beam.
• The film cassette has to be placed behind a protective metal shield. A narrow opening in this shield is required to allow a small part of the film to be exposed to the X-ray beam at any one instant.
• A cassette carrier, incorporating the metal shield, has to be linked to the X-ray tubehead to ensure that they move in the opposite direction to one another during the exposure. This produces the synchronized tomographic movement in the vertical plane.
• Within this carrier, the film cassette itself has to be moved in the same direction as the tubehead. This ensures that a different part of the film is exposed to the X-ray beam throughout the exposure.
The principle of narrow-beam linear tomography using this equipment is illustrated in Fig. 12.6.
Narrow-beam rotational tomography
In this type of tomography, narrow-beam equipment is again used, but the synchronized movement of the X-ray tubehead and the cassette carrier are designed to rotate in the horizontal plane, in a circular path around the head, with a single centre of rotation. The resultant focal trough is curved and forms the arc of a circle, as shown in Fig. 12.7.
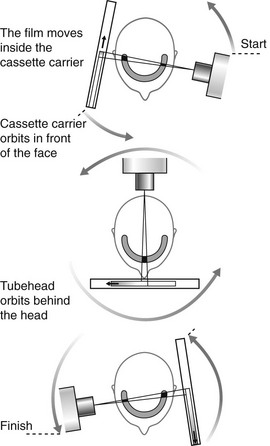
• The X-ray tubehead orbits around the back of the head while the cassette carrier with the film orbits around the front of the face.
• The X-ray tubehead and the cassette carrier appear to move in opposite directions to one another.
• The film moves in the same direction as the X-ray tubehead, behind the protective metal shield of the cassette carrier.
• A different part of the film is exposed to the X-ray beam at any one instant, as the equipment orbits the head.
• The simple circular rotational movement with a single centre of rotation produces a curved circular focal trough.
• As in conventional tomography, shadows of structures not within the focal trough will be out of focus and blurred owing to the tomographic movement.
Panoramic tomography
There are several dental panoramic units available; they all work on the same principle but differ in how the rotational movement is modified to image the elliptical dental arch. Four main methods (see Fig. 12.8) have been used including:
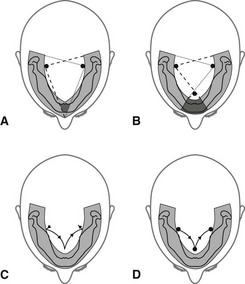
• Two stationary centres of rotation, using two separate circular arcs
• Three stationary centres of rotation, using three separate circular arcs
• A continually moving centre of rotation using multiple circular arcs combined to form a final elliptical shape
• A combination of three stationary centres of rotation and a moving centre of rotation.
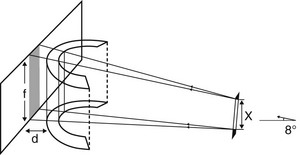
However, the focal troughs are produced, it should be remembered that they are three-dimensional. The focal trough is thus sometimes described as a focal corridor. All structures within the corridor, including the mandibular and maxillary teeth, will be in focus on the final radiograph. The vertical height of the corridor is determined by the shape and height of the X-ray beam and the size of the film, as shown in Fig. 12.9.
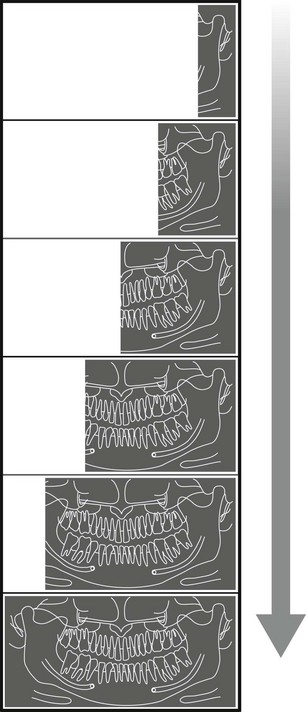
As in other forms of narrow-beam tomography, a different part of the focal trough is imaged throughout the exposure. The final radiograph is thus built up of sections (see Fig. 12.10), each created separately, as the equipment orbits around the patient’s head.
Selection criteria
• Where a bony lesion or unerupted tooth is of a size or position that precludes its complete demonstration on intraoral radiographs
• In the case of a grossly neglected mouth
• In assessment of periodontal bone support often supplemented with periapical radiographs
• For the assessment of wisdom teeth prior to planned surgical intervention. Routine radiography of unerupted third molars is not recommended
• As part of an orthodontic assessment where there is a clinical need to know the state of the dentition and the presence/absence of teeth. The use of clinical criteria to select patients rather than routine screening of patients is essential.
In addition, in dental hospitals panoramic radiographs are also used to assess:
Equipment
Although varying in design and appearance, all panoramic units consist of four main components:
• An X-ray tubehead, producing a narrow fan-shaped X-ray beam, angled upwards at approximately 8° to the horizontal (see Fig. 12.9)
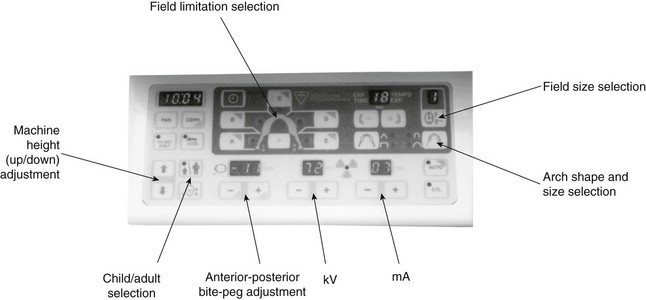
• Control panel (see Fig. 12.11)
• Patient-positioning apparatus, including chin and appropriate head immobilizing supports and light beam markers
• An image receptor (film or digital), with or without an associated carriage assembly.
Traditional panoramic equipment was designed to use indirect-action radiographic film in an extraoral cassette as the image receptor. With the advent of digital imaging several variations in image receptor now exist, including:
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


