Chapter 11
Other surgical procedures
Introduction
The most common indications for periodontal surgery are to access the root surfaces for debridement under direct vision or to carry out a resective or regenerative procedure (see < ?xml:namespace prefix = "mbp" />
• If the gingiva is partly or completely covering the crown of the tooth/teeth, surgical reduction of the gingiva may be needed to facilitate oral hygiene.
• If the gingiva is partly or completely covering the crown of the tooth/teeth, surgical reduction of the gingiva may be needed to access the tooth for restoration.
• To provide adequate sound supragingival tooth tissue to ensure restoration retention, and resistance without encroaching on the biologic width.
• To address aesthetic concerns, particularly when an excess of gingiva is shown.
This chapter discusses some of the surgical procedures used to manage these conditions.
Gingival procedures to remove excess gingiva (gingivectomy)
Gingival overgrowth is not an uncommon clinical finding, and there are a number of reasons why this might occur (
Table 11.1 Causes of gingival enlargement
Table 11.2 Advantages and disadvantages of different flap techniques for a gingivectomy
| Technique | Advantages | Disadvantages |
|---|---|---|
| Reverse bevel | ||
| Inverse bevel |
Case 1: Drug-induced gingival enlargement
A 36-year-old male patient presented with concern about his gums looking very swollen. Medical history revealed that he was diagnosed with hypertension 4 years ago, and he had been taking amlodipine 10 mg and bendroflumethiazide 2.5 mg per day. He reported that his “gum problem” started 1 year after initiating his medication.
The patient has been visiting his dentist regularly and has been receiving scaling without local anaesthesia every 6 months.
The attached and free gingiva were grossly overgrown and bled readily upon probing (

| 3 | 4 | 3 |
| 4 | 4 | 4 |
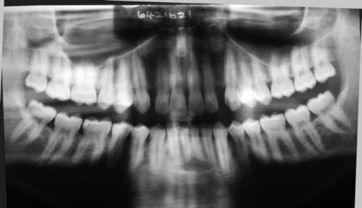
Little alveolar bone was evident on the panoramic radiograph (
The width of gingival tissue to be removed by the combination of these incisions is preplanned by “sounding out” the underlying bone crest and ensuring that a width of keratinized gingiva of at least 3 mm remains. To remove and thin the excess gingival tissue in this case, a gingivectomy was performed using an inverse bevel incision combined with an intracrevicular incision (
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


