Chapter 1
Resin Composites
Aim
The aim of this chapter is to improve understanding of the wide range of resin composites (including ormocers and ceromers) available for the restoration of anterior and posterior teeth.
Outcome
Readers will gain knowledge of the advantages and disadvantages of each of the many different types of resin composite materials available and how properties relate to material composition.
Introduction
Resin composites may be used to restore anterior and posterior teeth. When used anteriorly, aesthetics are often of primary concern, requiring durable high surface polish, excellent colour matching and colour stability. Posteriorly, where biting forces may be up to 600 N, high compressive and tensile strength and excellent wear resistance are required. Both anterior and posterior resin composites require a reliable bond to enamel and dentine to prevent leakage between the tooth and the restoration and to provide dimensional stability. Resin composites were first used in dentistry in the 1960s, and since then many different types of material have been developed for varying clinical indications.
Indications
Anterior Composites
Resin composite is used as a direct restorative material for the replacement of missing dentine and enamel. It is also used to alter the shape and colour of anterior teeth to enhance aesthetics. It can be used to close diastemas and alter crown length and contour, and it can be placed as a labial veneer to mask intrinsic discolouration and structural defects in a tooth.
Posterior Composites
Resin composite is also increasingly used as a direct restorative material for the replacement of missing dentine and enamel in posterior teeth. It is chosen as an aesthetic alternative to dental amalgam as a definitive restorative material for load-bearing occlusal and proximal preparations, for the restoration of tooth wear and as a core build-up material. It can also be used indirectly, to produce laboratory-made inlays and onlays that are then bonded to the prepared tooth using a resin composite luting cement and dentine adhesive systems. Increasing numbers of patients are requesting alternatives to dental amalgam in response to much-publicised concerns regarding the effects of mercury released from dental amalgam (see Chapter 5, pages 80–81, Safe use and disposal). Resin composite is not, however, an ideal restorative material in all clinical situations.
Composition of Resin Composites
Resin composite comprises resin matrix and glass filler particles, which polymerise (set) by chemical or light initiation. The glass filler particles are coated with a coupling agent to improve the bond to the matrix. In addition, initiators and accelerators are required for polymerisation. Inorganic oxide pigments are added in small amounts to achieve the various shades required.
Resin Matrix
Most resin composites are based on bisphenol-A-glycidyl methacrylate (bis-GMA) or urethane dimethacrylate (UDMA). Other resins used to alter viscosity and handling include triethylene glycol dimethacrylate (TEGDMA) and bisphenol-A-polyethylene glycol diether dimethacrylate.
Glass Filler Particles
Various filler particles are used by dental manufacturers, including silicon dioxide, aluminium oxide, barium, zirconium oxide, borosilicate and barium aluminium silicate glasses. The greater the amount of filler particles, the better the physical and mechanical properties of the material, up to a maximum level. Beyond this, the resin becomes too viscous to use clinically.
Filler particles give the following properties:
-
increased wear resistance
-
increased hardness
-
increased translucency
-
decreased polymerisation contraction
-
decreased coefficient of thermal expansion.
Resin composites may be classified according to the size and distribution of the filler particles (Table 1-1).
| Classification | Range of particle sizes (μm) | Filler (% by volume) |
| Hybrid | 0.04–3.0 | 60–70 |
| Microfill | 0.04–0.2 | 32–50 |
| Condensable (packable) | 0.04, 0.2–20 | 59–80 |
| Flowable | 0.04, 0.2–3.0 | 42–62 |
| Nanohybrid (nanocomposite) | 0.002–0.075 | 68–78.5 |
Coupling Agents
Silanes are the most commonly used coupling agents, for example 3-methacryloxypropyl trimethoxysilane (MPS). In many resin composites, the molecule has silanol groups at one end and methacrylate groups at the other. These molecules form covalent bonds to the silicon–oxygen groups of the filler particles and the methacrylate groups of the resin (Ferracane, 1995). When silane is deposited on the filler particle, the methoxy groups hydrolyse to hydroxy groups, which react with water or hydroxyl-radical groups on the filler. The carbon double bonds of the silane react with the resin and form a continuous bond between the filler particles and the resin matrix via the coupling agent. These bonds degrade when exposed to water intraorally (Powers and Sakaguchi, 2006).
Initiators and Accelerators
The majority of resin composites are light-cured. Polymerisation is initiated when the material is exposed to a blue light with a wavelength of around 470 nm. The light is absorbed by a photoactivator, often camphorquinone, which together with an aromatic amine initiates the polymerisation reaction.
Some resin composites are dual-cured, where polymerisation is commenced by exposure to blue light but the reaction continues after light exposure by the chemical reaction taking place between an organic amine and organic peroxide. This reaction produces free radicals, which react with the carbon double bonds of the resin, causing polymerisation and set of the material. Dual-cured resin composites are useful materials as core materials, where bulk placement may mean that light cannot penetrate to the full depth of the material, and thus the chemical reaction, which proceeds in the absence of light, ensures maximum polymerisation. They are also useful as luting agents for the cementation of all-ceramic crowns, porcelain-fused-to-metal crowns, posts and orthodontic brackets, all situations where full light penetration is not, or may not be, possible.
The amount of polymerisation, or degree of conversion of carbon double bonds to single bonds, varies: typically 65–80% when light-cured and 60–75% when chemically cured. Dual-cured materials may achieve up to 80% degree of conversion. The degree of conversion is clinically relevant because many of the physical and mechanical properties improve as it increases. The degree of polymerisation is affected by the length of time of exposure to the curing light, distance from the curing light, shade of composite, type of resin and filler composition.
The polymerisation reaction produces a net shrinkage of the material as the cross-linkage proceeds. The larger the volume of filler particles in a resin composite, the lower will be the shrinkage, thus microfilled composites, which have the lowest percentage volume of filler particles (Table 1-1), give the highest values of linear shrinkage: 2–3%. Hybrid composites have lower values of linear shrinkage: 0.6–1.4%.
Types of Resin Composite
Microfill Composites
Microfill resin composites are designed for use in anterior preparations, where aesthetics are the primary concern. Traditionally, they have very small silica filler particles, but the particles tend to agglomerate giving very low filler loading, and therefore low strength and wear resistance, and high polymerisation contraction, thermal expansion and water absorption. The small particle size provides good surface polish compared with resin composites with larger filler particles.
Hybrid Composites
Hybrid composites were developed as “universal” materials, with sufficiently good aesthetics to be used anteriorly but with sufficient strength and wear resistance to be also used posteriorly. Some hybrid composites are marketed specifically for posterior use. A typical hybrid composite material is shown in Fig 1-1.

Fig 1-1 Presentation of a typical hybrid resin composite restorative material, showing the enamel and dentine adhesive system, single-use compules, etchant, shade guide and applicator gun.
The clinical placement of a hybrid composite material in a distal cavity in an upper right central incisor tooth is illustrated in Figs 1-2 to 1-11.

Fig 1-2 Prepared cavity on distal aspect of upper right central incisor tooth. The tooth has been isolated with a rubber dam to prevent contamination of the dentine and enamel by saliva, gingival exudate or blood.

Fig 1-3 Prepared cavity with interproximal acetate matrix strip and wooden wedge in place. The wedge separates the teeth slightly to ensure a tight contact point between the new restoration and the adjacent tooth when the matrix strip is removed. The enamel and dentine of the cavity is then etched with orthophosphoric acid, rinsed and lightly dried.

Fig 1-4 Application of enamel and dentine adhesive to a small applicator brush from the product delivery system.

Fig 1-5 Enamel and dentine adhesive system is applied to the etched enamel and dentine with the small applicator brush.
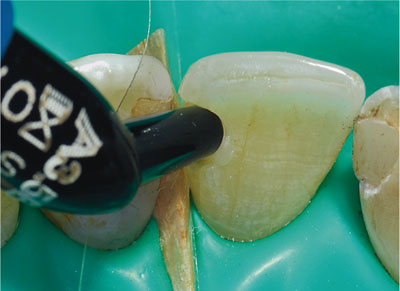
Fig 1-6 Syringing hybrid composite into cavity.

Fig 1-7 Tightly adapting matrix strip around tooth using finger pressure.

Fig 1-8 Photopolymerisation of hybrid composite material.

Fig 1-9 Newly placed composite restoration.

Fig 1-10 Polishing composite restoration with small-diameter aluminium oxide disc.

Fig 1-11 Finished hybrid composite material restoration.
Hybrid materials contain a range of particle sizes (Table 1-1), which permits higher filler loading and improved physical properties. The larger filler particles give a poorer surface polish than microfills, so they are not indicated where aesthetics are paramount. In recent years the trend has been to introduce increasingly smaller filler particles, in the spaces between the larger filler particles, to improve the surface polish and maintain filler loading. These materials are referred to as microhybrid resin composites. The most recent resin composites have continued the trend towards smaller filler particles with the use of fillers in the nanometre (10-9) range. These are referred to as nanohybrids or nanocomposites.
Nanocomposites
In general, nanocomposites are recommended for use in direct anterior and posterior restorations, core build-ups, veneers, splinting, inlays and onlays. A number of manufacturers produce nanocomposites; an example of a nanocomposite is shown in Fig 1-12. The main advantages claimed for incorporation of nanofillers are:
-
Higher filler loading, giving enhanced physical properties, without increasing viscosity to an unacceptable level.
-
High polish can be achieved and maintained long term, giving good aesthetics for anterior use.
-
Increased wear resistance.
-
Reduced volumetric shrinkage (1.5–1.7%) compared with other resin composite, aiming to reduce residual stress following photo-polymerisation.

Fig 1-12 A nanocomposite resin composite material, showing the shade guide, compules, enamel and dentine adhesive syst/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


