Dental Hygiene Care for Clients with Special Care Needs
General Considerations
Lifespan Approach to Care
A Principles of growth, development, and maturation
1. Growth includes physical and functional maturation
2. Growth is generally a continuous and orderly process but can be modified by numerous factors (e.g., nutritional deficiencies)
3. Different parts of the body grow and mature at different rates
4. Critical periods exist in growth and development
5. Hormonal changes can alter:
6. During growth and maturation, a person’s perception of self and that of self in relation to others change
7. Health status generally progresses from acute illness to chronic illness
8. Transition from one life stage to another is gradual and not necessarily based on chronologic age
B The U.S. health care system (see the section on “Providing oral health care” in Chapter 20)
1. The current system is categorical, with many gaps in services
2. A continuum of services through people’s life stages must ensure:
3. Health care providers should consider:
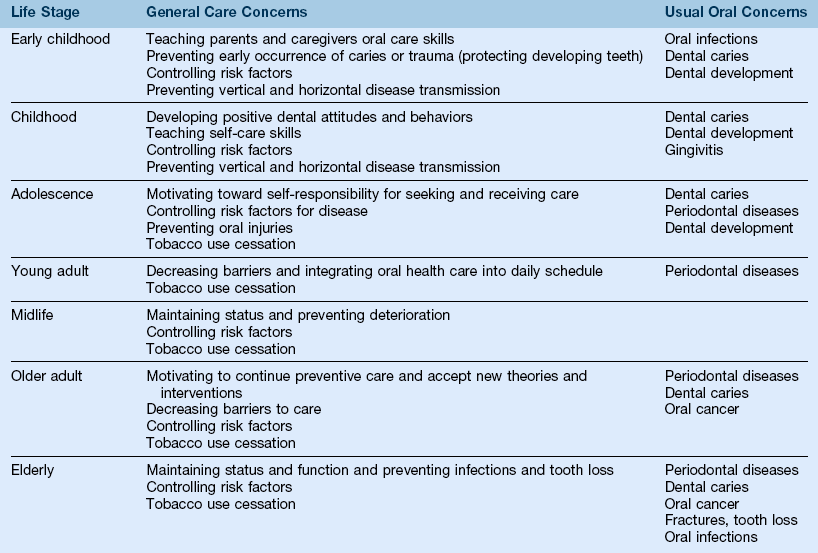
4. Oral health needs and approaches to care can differ throughout a person’s life cycle (Table 19-1)
Incidence and Prevalence of Individuals with Special Needs
A National statistics on incidence and prevalence figures are difficult to compile because of:
1. Unreliable reporting systems
2. Variable and changing definitions of conditions
3. Differences between acute conditions versus chronic conditions
B More than 60 million persons (1 in 5 persons) are considered disabled as defined by the Americans with Disabilities Act; of these, approximately 1 million are children younger than 6 years old
C In the United States, 32.5 million persons are considered to have a severe disability
D Table 19-2 identifies the most common chronic conditions in the older adult population
TABLE 19-2
Leading Chronic Conditions in the Older Adult Population
| Noninstitutionalized | Nursing Home Residents |
| Arthritis | Arthritis |
| Hypertension | Heart disease |
| Hearing impairments | Mental illness |
| Heart disease | Paralysis |
E The most common disabilities in the United States are caused by cardiovascular disease, back problems, arthritis, asthma, and diabetes
F The prevalence of disability increases with age
1. Of persons in the United States age 5 to 15, 6% are disabled
2. Of persons in the United States age 16 to 64, 12% are disabled
3. Of persons in the United States age 65 and older, 41% are disabled
G The most frequently reported chronic conditions that cause disability are diabetes, arthritis, cardiovascular disease, hypertension, cancer, spinal curvature, and back impairments
H Of individuals with developmental disabilities, 80% live in community-based residences or at home with families
The Dental Hygienist and Individuals with Special Needs
A Recognize physical, mental, medical, social, and oral needs
B Communicate with clients and caregivers in a positive, appropriate, nondiscriminatory manner
C Communicate with other professionals and team members to facilitate planning, implementation, and coordination of care
D Plan, implement, and evaluate community-based and office-based programs
E Adapt dental hygiene care plans, interventions, and evaluations to meet clients’ special needs, considering:
F Identify and eliminate potential barriers to care
G Assess one’s own attitudes, values, and commitment to provision of oral health services to these clients
H Evaluate local, state, regional, and national trends for their potential impact on the provision of oral health care
I Advocate oral health promotion and disease-prevention programs, full use of dental hygienists, and development of sound research so that evidenced-based care is provided in oral health care programs
General Definitions
These tend to change frequently and often overlap.
A Labeling—the process of classifying persons for educational, medical, or financial reasons
B Barrier-free environment—facilities that are physically accessible to everyone
C Normalization—making available patterns and conditions of everyday life that are as close as possible to the norms and patterns of mainstream society
D Mainstreaming—integration of persons with special needs into community-based programs and services
E Access to oral health care—opportunity for each individual to enter into the oral health care system and use the needed services
Potential Barriers to Oral Health Care
a. One fourth of the older adult population has an inadequate income level; percentages are higher for women, ethnic minorities, and single heads of households
b. Between 65% and 85% of disabled persons live near the poverty level
c. Medicaid coverage for oral health care is extremely variable across states and often does not cover older adult care
d. Medical and pharmaceutical expenses for many persons with disabilities consume a major portion of their incomes
e. Many individuals with special needs who have limited incomes cannot afford standard private practice fees for dental care, have no health insurance, or are underinsured
2. Transportation and geography
a. More than 50% of the disabled and older adult population lives in urban settings; the remainder lives in small rural communities or on farms
b. Public transportation is often unreliable, confusing, unaffordable, or nonexistent
c. Clients with special needs often rely on others for transportation to dental appointments, which increases their dependence and makes scheduling and compliance difficult
d. Homebound, hospitalized, or institutionalized clients frequently cannot be transported for care in the community
a. Minimum standards for accessibility must be met by dentists according to the Americans with Disabilities Act of 1993
b. External barriers include parking lots and spaces, walkways, curbs, stairs, narrow doors and entryways, heavy or pressurized doors, and small-print signs
c. Internal barriers include narrow passageways or doors, cluttered rooms or hallways, loose rugs or heavy shag carpets, abrupt changes in floor textures, noncontrasting colors, and bathrooms without grab-bars or other modifications
1. More than 50% of persons in the United States express positive attitudes toward older adults and persons with disabilities, and yet most really perceive them as “different” and “inferior”
2. Society perceives disabilities, differences, and disease states before recognizing similarities
3. Feelings of guilt, anxiety, apathy, inadequacy, embarrassment, depression, anger, and resentment about special needs interfere with attempts to seek care
4. Fear of or inability to comprehend dental procedures, antisocial or atypical behavior, or dependency on oral health care providers interferes with provision of care
5. Basic daily needs and activities are often overwhelming and can lower the priorities for oral health care
6. Perception of self-image and worth can affect care planning
C Provider philosophy and provision of care
1. The Americans with Disabilities Act requires that public and private dental offices serve persons with disabilities, that treatment is provided on the same basis as for nondisabled persons, and that dentists make reasonable modifications to facilitate access
2. Despite the Americans with Disabilities Act, surveys indicate that approximately 20% of dentists are unwilling to treat persons who are physically or mentally challenged
3. Reasons given for not treating individuals with special needs include:
a. Inadequate facilities and equipment
b. Inadequate training (knowledge and competencies)
c. Not wanting to expose “normal” clients to “special” clients
d. Inability to collect adequate fees
e. Additional effort and time required
f. Personal discomfort about perceived “differences” of special clients
g. Treatment of medically complex persons increases insurance premiums
D Communication and cultural concerns
1. Sensory impairments (hearing, visual) limit the client’s ability to transmit and receive communications when scheduling or undergoing oral care or participating in oral health care education
2. The use of technical terminology or inappropriate language level may interfere with understanding
3. Differences in communication styles (eye contact, physical proximity and contact, formal versus informal speech, cultural variations, use of nonverbal cues and verbal language) can impair effective communication
4. Use of condescending voice tones or language levels closes off communication lines
5. Foreign language barrier may deter a client from seeking care or reduce effectiveness of care
6. Inadequate numbers of health care providers possess cross-cultural competence
F Mobility and stability concerns
1. Impaired ambulation or use of assistive devices may hinder access to care
2. Uncontrolled or sudden movements may interfere with home care or dental hygiene interventions
3. Uncontrolled or aggressive behavior may endanger the care providers and the client
4. Spatial disorientation may interfere with client relaxation in the dental chair or with oral care procedures
Specific Conditions
See Chapters 8 and 9.
Intellectual and Developmental Disabilities (IDD)
1. Subaverage intellectual functioning originating during the developmental period and associated with impairment in adaptive behavior (formerly known as mental retardation)
2. Not the same as mental illness
B Incidence—2% to 3% of the U.S. population (57.7 million total), depending on criteria
D Etiology—acquired (12%), inherited (13%), unknown (75%)
1. Viral infections and toxemias (rubella, meningitis, lead poisoning)
2. Trauma and physical or chemical agents (child abuse; fetal alcohol syndrome)
3. Disorders of metabolism or nutrition (phenylketonuria—PKU)
4. Gross brain disease (atrophy or neoplasms)
6. Gestational disorders (Rh incompatibility, anoxia, prematurity)
E Signs, symptoms, and clinical manifestations
1. Variable, depending on etiology
2. Unusual difficulty in learning and applying what is learned to issues of daily living
3. Skull or other craniofacial anomalies may exist
a. Microcephaly—small cranium that restricts brain growth
b. Hydrocephaly—expansion of the cranium from excessive accumulation of cerebrospinal fluid
4. General developmental delays
5. Other possible manifestations include motor incoordination, visual or hearing disorders, specific learning disabilities, emotional disturbance, medical disabilities, seizure disorders
1. Most oral health problems are not inherent to the disability but are related to extrinsic factors (e.g., neglect by caregivers or lack of coordination leading to poor oral disease control)
2. Decayed-missing-filled surfaces (DMFS) scores comparable with those of the general population, but the “decayed” component may be higher because of lack of professional treatment (Figure 19-1)

3. Higher prevalence of periodontal conditions, probably related to poor oral hygiene and lack of regular care
4. Higher incidence of malocclusion and deviations in tooth eruption is associated with craniofacial syndromes or growth abnormalities (Figures 19-2 and 19-3)


5. Some instances of enamel dysplasia, more commonly seen in those with severe mental deficiencies resulting from severe prenatal or perinatal defects or insults
6. Some instances of physical self-abuse, if severely impaired
Fetal Alcohol Spectrum Disorders (FASD)
A Definition—an umbrella term describing a pattern of malformations caused by maternal alcohol consumption during pregnancy, characterized by prenatal and postnatal growth deficiency, dysmorphic facial features, and central nervous system (CNS) dysfunction including fetal alcohol syndrome (FAS), alcohol-related neurodevelopmental disorders (ARND), and partial fetal alcohol syndrome (PFAS)
1. Incidence of fetal alcohol spectrum disorders is 1 in 100 live births or 40,000 infants each year in the United States
2. Leading known preventable cause of mental impairments and birth defects in the United States
1. Severity of fetal alcohol effects is dose dependent
2. Babies with fetal alcohol syndrome are born to women who are “heavy drinkers” during pregnancy (usually at least 45 drinks per month)
3. Effects related to differences in blood alcohol content and differences in tissue susceptibility
4. Alcohol affects the cell membrane and cell migration, thus altering the organization of embryonic tissue
5. The fetal brain is most susceptible during the third trimester
6. Metabolic disturbances can retard fetal cell division and growth
D Signs, symptoms, and clinical manifestations
1. Premature or postnatal (or both) growth retardation—results in short stature, slight build, small head
2. Craniofacial dysmorphia—short eye openings, short upturned nose, smooth philtrum, flat midface, thin upper lip
3. Nonspecific abnormalities in any organ system, depending on the time of alcohol insult
4. Wide IQ range, many within the IDD range
5. Limited ability to read and write, but with minimal comprehension; also language problems
6. Poor social judgment and socialization skills
7. Hyperactivity and short attention span
E Treatment—depends on specific anomalies and organ systems affected
1. Surgery, if indicated for heart or other defects
2. Infant stimulation programs

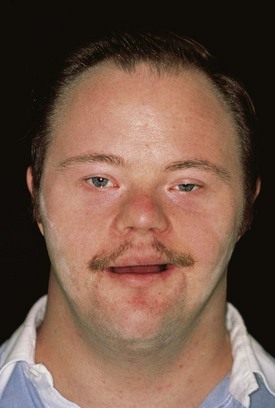
Down Syndrome
1. Mental or intellectual disorder
2. Associated with an anomaly of chromosome 21 (trisomy 21) in all or some body cells
B Incidence—most common chromosomal abnormality (1 in 800 live births; but varies with maternal age); approximately 400,000 individuals in the United States affected
C Signs, symptoms, and clinical manifestations
2. Poor muscular development, with hyperflexibility and hypotonia during childhood
3. Short stature, with delay in skeletal maturation
4. Short neck; extremities with broad stubby fingers
5. High incidence of congenital heart defects (30% to 50%); language, vision (60%), and hearing problems (75%); risk of leukemia (less than 1% out of 100), thyroid problems, and immunologic defects
D Oral manifestations (Figure 19-5)
1. Relative mandibular prognathism as a result of a small nasomaxillary complex
2. Dry skin and thick, dry, fissured lips
3. Open mouth posture, with a protrusive, fissured tongue
4. Hyperplasia of the adenoids and tonsils
5. Altered salivary gland mechanism (decreased flow)
6. Increased susceptibility to severe periodontal disease of early onset, especially in anterior areas; may be related to host immune defects (e.g., periodontitis as a manifestation of a systemic disease)
7. Delayed eruption of teeth and abnormal tooth development
8. Higher incidence of congenitally missing teeth
9. Small tooth crowns with short crown–root ratio
10. Enamel dysplasia (Figure 19-6)

11. Malocclusion—anterior open bite or cross-bite, posterior cross-bite, malocclusion common

Autism Spectrum Disorders (ASD)
1. A group of developmental disorders that affect the functioning of the brain, resulting in specific behavioral and communicative difficulties; speech, language and communication, social interaction, sensory impairments, play, and repetition of behaviors are key areas affected
2. Wide range of symptoms and behaviors with considerable individual variation
1. Incidence not completely known; prevalence rate of autism is increasing 10% to 17% annually
2. Unclear if the increase is real or reflects better diagnostic practices
3. Occurs in as many as 1 in 110 children
D Signs, symptoms, and clinical manifestations
1. Great variability in expression; no standard type
2. Extreme aloneness; failure to develop eye contact, to cuddle as infants normally do, to develop social relationships, or to perceive others’ feelings
3. Language disturbances—repetitious speech, pronoun reversals, lack of ability to use gestures; failure to develop functional speech in 50%
4. Comprehension problems, especially with verbal directions
5. Obsessiveness about maintaining routines and sameness of the environment (resistance to change)
6. Abnormal response to stimuli; may not respond to pain; or may have constant movement and repetitious activity
E Treatment—variety of approaches tried with varying success
1. Psychotherapy and behavioral therapy
4. Pharmacologic treatments include antipsychotics such as risperidone, stimulants such as methylphenidate hydrochloride (HCl), antidepressants, and tranquilizers
F Oral manifestations—none directly associated with the syndrome; difficult behaviors, feeding problems, and poor cooperation are challenges to dental care
Attention Deficit Hyperactivity Disorder (ADHD)
1. Developmental and behavioral disorder affecting specific areas of learning or impulse control that can cause problems in acquiring new skills
2. Relates primarily to vision, hearing, language, attention, and touch
1. Much controversy over diagnosis and treatment
2. Occurs in 7.8% of school-aged children; 4.5 million children aged 5 to 17 have been diagnosed in the United States
C Etiology—unknown, but may be related to:
D Categories—areas of CNS function affected
1. Input—receiving, recognizing, and decoding messages (e.g., auditory-perceptual or visual-perceptual problems)
2. Organization—information storage, integration with other information, and prompt retrieval (e.g., short-term memory problem)
3. Output—management of movement or utterances (e.g., hyperactivity, apraxia)
E Signs, symptoms, and clinical manifestations
1. Hyperactivity and inattentiveness
2. Irritability, impulsiveness, and need for immediate satisfaction
3. Problems with concentration and memory
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


