Introduction
Many psychological, social, and cultural factors influence parents’ motivation to seek orthodontic care for their children. In this study, we used Q methodology to identify and categorize shared motives and determine whether cultural differences exist between Hispanic/Latino (H/L) and non-Hispanic/Latino, white (W) parents.
Methods
The fundamental question posed to the parents was “Why do you want your child to have braces?” Q methodology involves 3 stages. (1) Interviews of H/L (n = 5) and W (n = 5) parents generated 35 statements that represented different motives to seek orthodontic care. (2) In the Q sort, 70 new parents (22 H/L, 48 W) ranked statements in order of relative importance using a forced distribution grid. (3) Factor analysis was performed separately for the H/L and W groups to uncover cultural differences.
Results
Four motivational profiles were described for both the H/L and W parents based on the significant factors identified in each group. More H/L parents (18 of 22 parents) than W parents (22 of 48 parents) were characterized by 1 of their group’s 4 profiles. Comparisons of the motivational profiles across the groups showed 4 global themes: well-timed treatment that prevents future dental problems, parental responsibility, perceived benefits, and perceived need instilled by the dentist.
Conclusions
Four global themes captured the motives of most parents seeking orthodontic treatment for their children. Understanding these global themes can help clinicians frame their treatment discussions with parents.
Highlights
- •
Four motivational profiles for Hispanic and white parents were identified.
- •
Hispanic parents were more likely to be characterized by 1 of the 4 profiles.
- •
Global themes capture the motives of most parents seeking treatment for children.
For many parents, the decision to seek orthodontic treatment for their child is multifactorial. Combinations of psychological, social, and cultural factors influence their motivation to pursue care. Although previous studies have investigated the factors that motivate parents, few studies have attempted to explain the significance of these motives and how they impact orthodontic treatment.
Recently, Prabakaran et al used a systematic approach known as Q methodology to investigate parents’ and patients’ motivations for orthodontic treatment in the United Kingdom. Q methodology has been applied previously in medicine, nursing, social sciences, and health education to explore matters of perspective. Prabakaran et al identified and described several shared viewpoints among parents that explained why they sought treatment. Interestingly, they found that more nonwhite parents (including all parents of “other races”) were motivated by a feeling of parental responsibility to seek orthodontic care for their children compared with their white counterparts. Their study emphasized the need for further research that includes other cultures and demonstrated that Q methodology is an effective tool to examine motivations for orthodontic treatment. Before the study by Prabakaran et al, only 2 orthodontic studies used Q sorting (part of Q methodology) to evaluate appearance, and neither study included factor analysis.
Our study was undertaken to better understand the subjective motives of parents who were seeking orthodontic treatment for their children and to examine potential cultural differences in their motivation. Q methodology uses qualitative and quantitative analyses to objectively compare the subjective human experience, systematically identifying a population’s shared viewpoints or opinions. If shared viewpoints can be described in this study, orthodontists may better understand how psychological, social, and cultural factors influence the decision to seek treatment. It may also facilitate the development of culturally appropriate strategies designed to improve communication and treatment planning. We aimed to identify and categorize motivational profiles (ie, shared viewpoints among parents) that explain the reasons that Hispanic or Latino (Hispanic/Latino) and white parents seek orthodontic treatment for their children and to determine whether there are differences between the parent groups.
Material and methods
The study participants consisted of Hispanic/Latino and non-Hispanic/Latino, white (white) parents whose children were seeking orthodontic care. The sex of the parent participating in this study was not recorded. The Hispanic/Latino Americans were compared with whites because they are the second largest ethnic group in the United States, with a significant representation in Washington state. Parents were recruited from the University of Washington’s Department of Orthodontics and Center for Pediatric Dentistry in Seattle.
Recruitment occurred in the clinical setting when the parents accompanied their children to an initial orthodontic examination or consultation. To be eligible for this study, parents had to meet 2 criteria: (1) the parent self-identified with the Hispanic/Latino or white racial or ethnic group, and (2) the child was between the ages of 8 and 16 years. Parents were excluded if their child was referred for orthognathic surgery or had any syndromes or developmental disorders. Consent was obtained from parents before enrollment in the study. Participants were compensated with a gift certificate after participation. All study procedures and materials were approved under exempt status by the Human Subjects Division at the University of Washington.
Consistent with the Q methodology framework, this study was conducted in 3 stages: (1) development of the statements (concourse) about the topic and the final Q set, (2) ranking of the statements in the Q sort, and (3) factor analysis and interpretation. The fundamental question the parents were asked was “Why do you want your child to have braces?”
Questions answered by the Q methodology ask “What is the nature of a view or belief in a particular population on a certain subject” rather than “What is the extent of those views or beliefs on that subject.” The ability of Q methodology to uncover patterns for how and why subjects have particular viewpoints rather than quantifying the percentage of people with a particular viewpoint makes it valuable when asking subjective questions. Factor analysis “identifies a group of persons who have rank ordered the provided items in a very similar fashion or, in other words, a group of persons who share a similar perspective…about the topic.” The factors become amenable to interpretation, representing narratives that explain the shared perspectives in the population. The distinctive characteristics of Q methodology related to sampling, validity, and reliability have been published previously.
Stage 1: concourse and final Q set
To develop a concourse that adequately represents the perspectives of Hispanic/Latino and white parents regarding their motivation to seek orthodontic treatment for their children, statements were generated from brief open-ended interviews with the parents. Participants were asked to describe why they sought orthodontic treatment for their children, based on the question “Why do you want your child to have braces?” Interviews were conducted by the primary author (B.B.D.). When necessary, a Spanish interpreter was available. Parent responses were manually recorded verbatim. After 10 interviews with Hispanic/Latino (n = 5) and white (n = 5) parents, the responses reached the point of saturation, and no new statements were generated. The statements were compressed by deleting duplicate statements and combining similar statements. Compression of the concourse resulted in 35 distinct statements that formed the final Q set. For the final Q set of distinct statements, 2 or more participants had provided the same response.
Stage 2: Q sort
The sample size estimation was based on the guidelines of Watts and Stenner, who recommended strategic (or purposeful) sampling of a smaller number of participants to capture particular viewpoints. As they explained, the participant group, or P set, should be selected with care so that they represent “participants whose viewpoint matters in relation to the subject.” Additionally, participant numbers in the P set were based on recommended guidelines of fewer participants than the number of items in the Q set. As further suggested, most P sets include participant numbers ranging from 40 to 60.
For the Q sort activity, new Hispanic/Latino and white parent participants (different from those previously interviewed) were recruited using the same recruitment procedure and inclusion and exclusion criteria as described above. If the parent was willing to participate, a link was sent to his or her e-mail address. In total, 128 parents were enrolled.
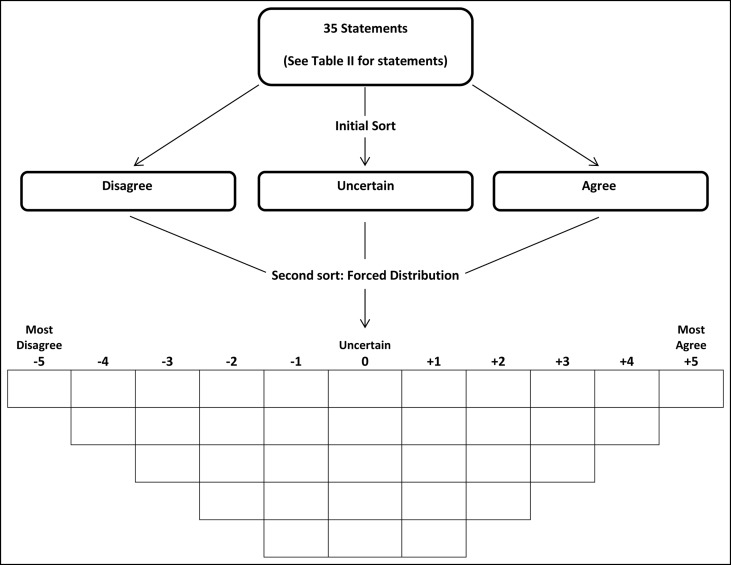
The Q sort task relies on a forced distribution Q methodology grid, the continuum of preference, which resembles a quasi-normal distribution; fewer statements can be placed at the extreme ends of the grid, and more statements are admitted in the middle “neutral” section. For this study, the Q sort was performed using an Internet application called Q-Assessor ( q-assessor.com ). When compared with traditional paper sorting, online Q sorting with Q-Assessor has been shown to be reliable and valid. In the Q-Assessor approach, the researcher inputs the statements (final Q set) to be used in the Q sort task, inputs and configures the bins (“the conceptual structure”) into which the statements are sorted, and configures the interface approach (button or drag-and-drop interface). The sort bins “define the ranked groupings into which subjects sort statements. Each bin contains a certain number of statements, has a certain numerical value used to calculate the study factor, and has a descriptive label.”
In this study, the 35 statements in the final Q set were available in English and Spanish. All statements were translated by a native Spanish speaker, with back-translation done to confirm proper translation. There were 11 sort bins ranging from “most disagree (−5)” to “most agree (+5)”; the neutral midpoint (0) was designated as “uncertain.” Study participants were presented with the question “Why do you want your child to have braces?” The parents were asked to complete 2 sorts of the 35 statements; the initial sort asked them to “drag and drop” each statement into 1 of 3 boxes (agree, disagree, or uncertain), and the second sort asked them to “drag and drop” each statement in the 3 boxes into the forced distribution grid based on where they thought the statement belonged ( Fig ). The parents were asked to fill the “most agree” bin first, then the “most disagree” bin, and then the remaining bins. The Q sort was complete after the participants placed all 35 statements in the sort bins on the grid. After the Q sort, the parents were asked, “How would you describe your race or ethnicity: Hispanic/Latino or white (non-Hispanic)?” A bilingual research assistant (A.P.) was available to answer questions and assist the Hispanic/Latino parents on the Q sort process.
Stage 3: factor analysis and interpretation
Factor analysis was performed with the Q-Assessor program. Factor analysis creates factors that represent clusters of participants with similar opinions and viewpoints. The Q-Assessor program can display the unrotated (using the centroid method) and rotated (either varimax or manual) factor structures. For this study, separate factor analyses were conducted for the Hispanic/Latino and white parents’ Q sorts using the varimax rotation method. Varimax rotation was used to maximize variance between factors; ie, it identifies Q sorts that are close to the viewpoint of a specific factor. The study team deemed factors significant if their eigenvalues were greater than 1 and at least 3 parents’ Q sorts mapped onto the factor.
Q-Assessor can generate reports that include tables and summaries of the factor scores to assist with interpretation. For this study, factor arrays were generated to indicate the relative position of each statement for each significant factor and identify which statements distinguish or do not distinguish (ie, consensus) the significant factors. The factor array is a composite Q sort that represents how a participant who loaded to a particular factor would rank the statements. The numeric values are weighted means of the participants who mapped to each significant factor. To better inform the interpretation, factor interpretation crib sheets were created from factor arrays for each significant factor based on methods described by Watts and Stenner. The crib sheets provided an organization framework from which to understand the ranking of the statements within a factor relative to the other factors. All significant factors were described, including statements with which parents agreed or disagreed were reasons for seeking orthodontic treatment for their children.
Results
As previously described, the final Q set was composed of 35 distinct statements derived from parent interviews during the first part of the study. Of the 128 enrolled parents for the second part of the Q methodology study, 70 parents (54.7%) completed the Q sorts. Of those 70 participants, 22 participants were Hispanic/Latino (31.4%) and 48 were white (68.6%).
The initial factor analysis showed that the unrotated factor matrix for Hispanic/Latino parents yielded 4 factors, whereas the matrix for white parents yielded 6 factors. After varimax rotation, 4 factors in each group were deemed significant. Table I shows the Q-Assessor factor analyses after varimax rotation for the Hispanic/Latino and white parent participants, including the significant factors after rotation, associated eigenvalues, percentage of variance accounted for by each factor, and the number of parents’ Q sorts that mapped to each factor. Not all parents mapped to 1 of the 4 significant factors in the Hispanic/Latino and white groups. Table II shows the factor arrays (composite Q sorts) of the Hispanic/Latino and white parents that mapped to each factor and how statements were ranked relative to the other factors. Table II also shows distinguishing and consensus statements among the Hispanic/Latino and white parents. For interpretation, the significant factors were named “parent-motivational profiles.”
| Hispanic/Latino parents (n = 22) | White parents (n = 48) | |||||||
|---|---|---|---|---|---|---|---|---|
| Factor | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 |
| Eigenvalue | 3.8 | 1.9 | 2.3 | 2.5 | 4.1 | 6.3 | 4.5 | 6.1 |
| % of total variance | 17.1 | 8.5 | 10.5 | 11.4 | 8.6 | 13.1 | 9.3 | 12.8 |
| Number of parents mapped to factor ∗ | 7 | 3 | 4 | 4 | 4 | 6 | 4 | 8 |
∗ Not all parents were mapped to the 4 significant factors resulting from the varimax rotation analysis.
| Statement | Hispanic/Latino factor rank | White factor rank | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 (n = 7) | 2 (n = 3) | 3 (n = 4) | 4 (n = 4) | 1 (n = 4) | 2 (n = 6) | 3 (n = 4) | 4 (n = 8) | ||
| 1 | Without braces, my child is defined by poor teeth | −2 | 0 | −1 | −1 | −3 | −1 | −1 | 0 |
| 2 | Braces improve my child’s ability to chew and function | 3 | 2 | −1 | −1 | −1 | 3 | 2 | 1 |
| 3 | I’m worried about gum problems | 1 | −1 ∗ | 1 | −4 ∗ | 2 ∗ | −2 | −1 | −1 |
| 4 | My child’s midline is off to one side † | 0 | −2 | 0 | 0 | −2 | −1 | 2 | −5 ∗ |
| 5 | My child’s friends have braces | −3 | 0 | 0 | −2 | 2 | −4 | 0 | 2 |
| 6 | Braces will help with jaw problems (eg, temporomandibular joint) ‡ | 1 | −2 | −2 | 1 | 0 | 1 | 1 | 0 |
| 7 | My child wants braces | −2 ∗ | 1 | 2 | 1 | 0 | −5 ∗ | 2 | 2 |
| 8 | I want to improve the appearance of my child’s face | −1 | −3 | −5 ∗ | 0 ∗ | −3 | −1 | 1 | 1 |
| 9 | I want my child’s teeth to last as long as possible † | 3 | 2 | 3 | 2 | 4 | 2 | 4 | 5 |
| 10 | Improve my child’s health † | 2 | 4 | 2 | 4 | 3 | 2 | 1 | 3 |
| 11 | Improve my child’s smile | 0 ∗ | 3 | 4 | 5 | 0 | −2 ∗ | 3 | 3 |
| 12 | Dentist or physician recommended braces | 4 | 5 | 3 | 0 ∗ | 5 ∗ | 3 | 0 | 2 |
| 13 | Braces have a social benefit | −2 | −1 | 4 ∗ | −1 | −2 | 0 | −2 | −2 |
| 14 | I want to improve my child’s confidence | 1 ∗ | 3 | 3 | 3 | 0 | 1 | 1 | 4 ∗ |
| 15 | Overbite | −1 | 0 | −4 | −3 | −1 | 4 ∗ | −1 | 0 |
| 16 | My child notices that things are uneven and wants straight teeth † | 2 | 2 | 2 | 2 | 1 | −2 | 4 | −1 |
| 17 | It’s a rite of passage to have braces | −3 | 0 ∗ | −2 | −4 | −2 | −3 | −4 | −1 |
| 18 | My child has oral-motor issues | 0 | 2 | −3 | −2 | −5 | −1 | −2 | −3 |
| 19 | I have problems with my teeth, and I don’t want my child to have problems | 4 ∗ | 1 | 1 | −3 ∗ | −1 | 1 | 3 | −3 |
| 20 | Braces are best when my child is growing ‡ | 3 | 0 | 0 | 1 | 1 | 2 | 0 | 2 |
| 21 | I had braces myself | −3 | −4 | −3 | −5 | 3 | −4 | −5 | −4 |
| 22 | My child has a crossbite | 1 ∗ | −3 | 2 ∗ | −3 | −3 | 1 | −1 | −3 |
| 23 | Braces have a cosmetic or esthetic benefit | 2 | −3 ∗ | 1 | 3 | 1 | 0 | −1 | 1 |
| 24 | Facilitates better hygiene | 1 | 4 ∗ | 0 | −1 | 0 | 0 | 0 | 1 |
| 25 | Crooked teeth | −1 ∗ | 1 | 1 | 1 | 3 | 2 | 1 | −1 ∗ |
| 26 | Tooth pain | −2 | −5 ∗ | −1 ∗ | −2 | −4 | −3 | −4 | −2 |
| 27 | It’s the responsibility of the parents to take care of their child’s health needs and issues ‡ | 5 | 3 | 1 ∗ | 4 | 4 ∗ | 3 | 2 | 3 |
| 28 | Prevent future problems | 2 | −1 ∗ | 5 ∗ | 0 | 2 | 4 | 5 | 4 |
| 29 | There’s not enough space for my child’s permanent teeth | 0 | −1 | −2 | 2 ∗ | 1 | 5 | −3 | −1 |
| 30 | I want my child to be equal to others | −4 | −1 | −2 | 0 | −1 | 0 | 0 | 0 |
| 31 | My child is teased | −4 | −2 | −4 | −2 | −4 | −2 | −3 | −4 |
| 32 | Braces are popular for children ‡ | −5 | −4 | −3 | −1 | −1 | −3 | −2 | −2 |
| 33 | My significant other or I want my child to have braces | −1 | 1 | −1 | 1 | 2 | −1 | −2 | 1 |
| 34 | Appearance of the teeth matters when getting a job | −1 | −2 | 0 | 3 ∗ | 1 | 1 | 3 | 0 |
| 35 | I’m concerned about injury to the front teeth † ‡ | 0 | 1 | −1 | 2 | −2 | 0 | −3 | −2 |
∗ Statements that distinguish a factor from the other 3 factors with Hispanic/Latino and white groups.
† Statements in which there is consensus (not distinguishable from other factors) among Hispanic/Latino parents.
‡ Statements in which there is consensus (not distinguishable from other factors) among white parents.
Hispanic/Latino parent profiles
Of the 22 Hispanic/Latino parents who participated, 18 (82%) mapped to 1 of the 4 motivational profiles, suggesting that the Hispanic/Latino participant population shared relatively similar reasons for seeking orthodontic treatment and probably a similar perspective of orthodontic treatment. Table III shows the narratives for the 4 significant Hispanic/Latino motivational profiles, described as (1) feeling of parental responsibility instilled by a dental professional; (2) perceived oral health needs, identified by a dental professional; (3) prevention of future problems, perceived benefits, or child’s motivation; and (4) esthetic benefit to improve the child’s self-image.


