Mesially tilted or impacted mandibular molars cause occlusal disharmony and periodontal problems. For proper restoration of the occlusion and to prevent further periodontal damage, uprighting of tilted molars is the recommended treatment option. Although several orthodontic methods including miniscrews have been proposed, most of them have innate limitations and problems such as the possibility of unwanted tooth movement. In this case series, we introduce a new system that uses 2 miniscrews with slots that can accommodate rectangular orthodontic wires to 3 dimensionally control the tilted molar in 3 patients. We also discuss the advantages and possible disadvantages of this new system.
Highlights
- •
This article introduces a new system that 3 dimensionally controls the tilted molar.
- •
The advantages and possible disadvantages of this new system are discussed.
Mandibular second molar impaction occurs in 3 of every 1000 people in the general population and in 2 or 3 of every 100 orthodontic patients. It is more common in male patients and most typically occurs unilaterally on the right side in the mandible rather than in the maxilla. Mandibular second molar impactions occur in several patterns: unilateral or bilateral, with or without loss of the mandibular first molar, and with or without mandibular third molar impaction. Many causative factors contribute to the abnormal eruption of the mandibular second molar: lack of arch length, abnormal erupting angulation, premature eruption of the mandibular third molar, early loss of the mandibular first molar, alteration of the dental follicle or the periodontal ligament, and other iatrogenic factors.
To obtain proper occlusion and prevent further periodontal problems, uprighting of mesially tilted molars is the recommended treatment and should be done as soon as possible. If not properly corrected, mesially impacted molars may lead to adverse events such as elongation of opposing teeth, periodontal problems on the mesial side of the affected teeth, caries in the unerupted molars, and poor oral hygiene. Many clinical procedures have been reported to upright mesially tilted mandibular molars, but biomechanical shortcomings have been observed. A disadvantage of uprighting mandibular molars with conventional dental anchorage is the unintended displacement of the anchorage tooth or teeth. To minimize dental anchorage displacement, it was necessary to include multiple teeth in the anchorage unit, which resulted in the placement of heavy orthodontic appliances.
During the last decade, the use of skeletal anchorage has been widely accepted in clinical orthodontics. Skeletal anchorage reduces the side effects that occur with dental anchorage and simplifies the orthodontic appliances and the treatment biomechanics. In this article, we introduce a biomechanical system for uprighting mandibular molars with 2 miniscrews and a connecting wire, and present 3 patients whose mesially tilted mandibular second molars were corrected with the system. This system was designed to provide a simple and efficient molar uprighting technique that will minimize the orthodontic appliances and be more comfortable for patients.
The technique uses 2 miniscrews with a slot that can accommodate an orthodontic wire (0.0215 × 0.0250 in) ( Fig 1 ). Machined-surface miniscrews (Dual Top Anchor System, JD type; Jeil Medical, Seoul, Korea) were 6 mm in length and 1.6 mm in diameter. The miniscrews were implanted in the attached gingiva between the mandibular first and second premolars, and between the second premolar and the first molar. A standard implantation method was used. Briefly, the surgical site was scrubbed with povidone-iodine, and local anesthesia was induced by infiltration with 2% lidocaine plus epinephrine (1:100,000). Then a miniscrew was implanted at 90° to the cortical surface using a manual driver under saline solution irrigation. A rectangular wire was used to connect the 2 miniscrews and move the target tooth. Connecting the 2 miniscrews provides effective resistance against orthodontic forces and moments that act to loosen the miniscrew (ie, loosening the moment force of one miniscrew acts to tighten the moment force of the other miniscrew, thereby neutralizing the forces). By placing a connecting wire in the 2 miniscrew slots, it is possible to create a 3-dimensional vector control force on the target tooth. The slots assume a role similar to that of orthodontic brackets that use conventional orthodontic mechanics to upright molars. The wire was placed immediately after miniscrew implantation.

Patient 1
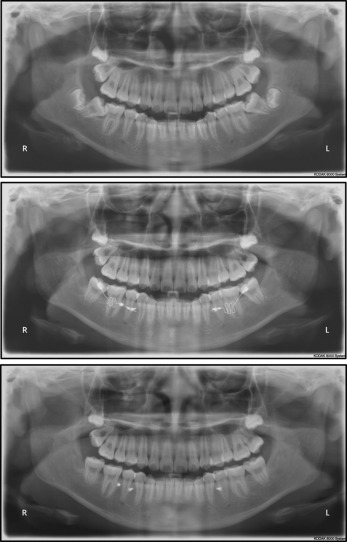
An 11-year-old girl presented with mesially tilted mandibular second molars on both sides. The clinical examination showed a Class I molar and canine relationship without notable arch length discrepancies ( Fig 2 ). Developing mandibular third molars were observed bilaterally on the panoramic radiographic view.

A treatment plan was established to upright both mesially tilted second molars using the 2-miniscrews system and to extract the mandibular left and right third molars to aid in uprighting the second molars. The occlusion and the alignment of the patient’s other teeth were fairly acceptable, and we did not plan to bond or band orthodontic appliances to keep their positions.
Two miniscrews on each side were implanted between the first molar, the second premolar, and the first premolar. An orthodontic tube was bonded on the mesially tilted second molars at the proper position. Initially, a passively bent 0.016 × 0.022-in stainless steel connecting wire was inserted into the 2 miniscrew slots and the second molar tube. A nickel-titanium open-coil spring was used for the distalization of the mandibular second molars ( Fig 3 ). After a month, both mandibular second molars were unlocked from the first molars, and a 0.017 × 0.025-in beta-titanium alloy wire with a loop was placed to upright the molars ( Fig 3 ). The miniscrew implanted between the left second premolar and the first molar fell out before application of the initial force; therefore, we decided to use 1 miniscrew on the left side instead of implanting another ( Fig 3 ). This 1 miniscrew withstood the orthodontic forces throughout the treatment.

After 9 months of treatment, the mesially tilted second molars were successfully uprighted, and the orthodontic tubes and miniscrews were removed ( Fig 3 ). The patient’s occlusion and dental alignment were maintained. After a year, the retention records showed that the alignment continued to be maintained ( Figs 3 and 4 ).
Patient 2
This patient was a 13-year-old girl with a malpositioned mandibular right second molar. The intraoral examination showed a Class I molar and canine relationship with good alignment of the maxillary and mandibular dentitions. Her mandibular right second molar was horizontally impacted with supragingival exposure of the distal part of the crown ( Fig 5 ). A panoramic radiograph showed horizontal impaction of the mandibular right second molar and absence of the third molars.
A treatment plan was established to upright the horizontally impacted mandibular right second molar using the 2-miniscrew system. One miniscrew was inserted between the first molar and the second premolar, and the other between the first and second premolars. An orthodontic half tube was bonded on the impacted second molar. A 0.016 × 0.022-in beta-titanium alloy looped spring was inserted to provide a distalization force to the impacted tooth ( Fig 6 ). An additional miniscrew was implanted on the distal side of the impacted tooth to aid the distalizing movement ( Fig 6 ). Two miniscrews and a connecting wire system were expected to be sufficient to normalize the position of the impacted tooth, but to enhance the efficiency of the applied force vector and thereby shorten the treatment time, an additional miniscrew was used. The third miniscrew was considered necessary to correct a severely horizontal impacted second molar. The more horizontally impacted the molar, the smaller the moment generated by the appliance. To increase the moment, it was decided to use both a pushing force from the buccal 2-miniscrew system and a pulling force from the ramal miniscrew ( Fig 7 ). However, experience with a series of similar cases had demonstrated that this additional miniscrew in the ramus is not necessary. The buccal 2-miniscrew system generates a couple moment in the molar tube, whereas the crown distal force generates a moment that uprights the second molar ( Fig 8 ). These moments were enough to upright a severely horizontal impacted second molar without a third ramal miniscrew (see patient 3, below). If the pulling force from a ramal miniscrew is desired, a modified design of the wire can be used ( Fig 9 ).
After 6 months, the half tube was replaced by a full-sized tube, and a 0.017 × 0.025-in beta-titanium alloy wire with loops was inserted to control the second molar ( Fig 6 ). After 8 months of treatment, a 0.016 × 0.022-in stainless steel wire was used for fine alignment of the second molar.
After treatment, the horizontally impacted second molar was uprighted successfully without interrupting the initial occlusion or the alignment of the other teeth ( Fig 6 ). The total duration of treatment was 13 months.
The retention records after 1 year showed that the treatment results were well maintained ( Figs 6 and 10 ).
Patient 2
This patient was a 13-year-old girl with a malpositioned mandibular right second molar. The intraoral examination showed a Class I molar and canine relationship with good alignment of the maxillary and mandibular dentitions. Her mandibular right second molar was horizontally impacted with supragingival exposure of the distal part of the crown ( Fig 5 ). A panoramic radiograph showed horizontal impaction of the mandibular right second molar and absence of the third molars.


