Fig. 2.1
Schematic diagrams of alveolar ridge augmentation. (a) Veneer bone graft, (b) onlay bone graft, (c) saddle bone graft, (d) interpositional bone graft, (e) ridge splitting technique
.
Bone restoration capability differs according to the method applied. Guided bone regeneration is restricted in terms of small feasible bone regain amount. When applied with resorbable membranes, the expected bone regeneration does not exceed 3–4 mm vertically and 4 mm horizontally. Titanium mesh may enhance the capability to 4–7 mm vertically and 5 mm horizontally. Onlay block bone graft has similar capability with the latter of GBR technique. Interpositional bone graft is capable of regaining 5–7 mm of vertical height. Distraction osteogenesis is the most capable modality in terms of feasible bone regain amount which may exceed 10 mm in vertical height and 6 mm in alveolar width.
2.2 Autogenous Block Bone Grafting
Autogenous bone graft had been the gold standard of bone grafting. It is the only graft material that is considered to have osteoconductive, osteoinductive, and osteogenetic properties all together. Furthermore when block bone is adapted properly, it may contribute to initial stability of the implant fixture installed simultaneously. This characteristic can increase the feasibility of simultaneous bone grafting and implant installation.
2.2.1 Autogenous Bone Donor Sites
Autogenous bone is harvested from either an intraoral site or extraoral. Intraoral donor sites include the chin bone, the ramal bone, the mandibular body window bone, the mandibular torus bone, the maxillary torus bone, the sinus anterior wall and the maxillary tuberosity bone. The chin bone is the most abundant source among the listed (Figs. 2.2 and 2.3).
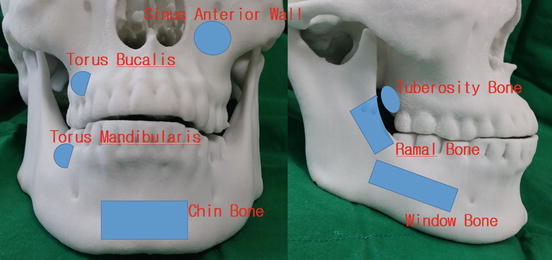
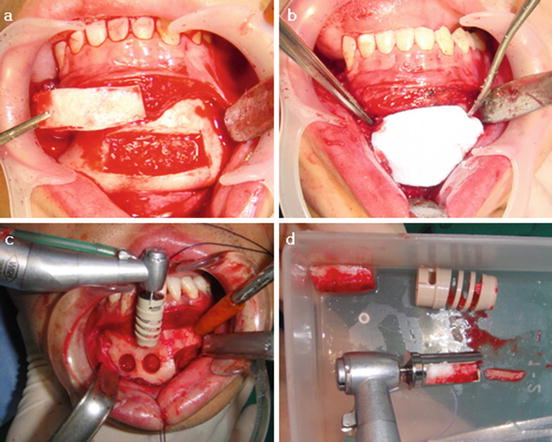
Fig. 2.2
Schematic diagram of the intraoral donor sites of autogenous bone
Fig. 2.3
Chin bone harvesting. (a) Window type block bone harvesting, (b) Barrier membrane placed for bone healing of the donor site, (c and d) Mushed particulated bone block harvesting with bone mill bur (Neobiotech®)
Extraoral donor sites include the anterior iliac crest bone, the proximal tibia bone, and the calvarial bone. These sites may suffice any amount of requisite for an alveolar augmentation.
2.2.2 Block Bone Grafting Techniques
The most intuitive form of autogenous block bone grafting is the onlay or veneer grafting techniques (Fig. 2.4).

Fig. 2.4
Case presentation of a veneer bone graft. (a) Edentulous state on the anterior maxilla with atrophic and narrow alveolar ridge and the flap design, (b) Veneer bone graft positioned and fixed with titanium screws, (c) Implant installation, (d) Final prosthetic outcome
These techniques directly replace the resorbed alveolar bone in a vertical or horizontal direction, respectively. Both vertical and horizontal augmentations are possible by the saddle bone graft technique. Khoury demonstrated the method and results of sinus floor augmentation with mandibular block bones where dental implants were installed simultaneously [1]. Cases with severely atrophic alveolar ridge may require additional bone grafting. In the atrophic maxilla, subnasal or subantral block bone graftings are applied in addition of the onlay bone graft for this purpose.
Vertical interpositional bone graft is an alternative to the conventional methods described above, when the bone demand is large. This method has the advantage of preserving the alveolar crest with intact nourished bone. Soft tissue management and flap design is very important and should be done carefully with interpositional bone graft procedures for preserving the vascularity.
2.2.3 The Fate of Autogenous Onlay Bone Graft
Resorption of grafted autogenous bone is always a matter of concern. Cordaro et al. reported that when block bones harvested from the mandibular ramus or symphysis are grafted in an onlay style, mean resorption rates during a graft healing period of 6 months were 23.5 % for lateral grafts and 42 % for verticals [2]. Proussaefs et al. suggested that vertical augmentation of the alveolar ridge with autogenous block bone from the mandibular ramus is a viable treatment option. They reported a vertical resorption rate of 16.34 % from an initial 6.12 mm of augmentation after 4–6 months of healing period [3]. Widmark et al. demonstrated that the horizontal resorption was 25 % after 4 months and 60 % at the time of abutment connection when symphyseal block bone was grafted to the anterior maxilla for single tooth implant installation [4].
In a clinical survey conducted in our department, 76 patients underwent simultaneous autogenous onlay bone graft and installation of total 256 dental implants from 2000 to 2006. The amount of bone augmentation was 5.42 mm in average. After a minimum follow up period of 2 years, average bone resorption at the mesial and distal site of implant collar was 1.48 mm. About 27.3 % of the augmented bone height was resorbed.
2.2.4 Drawbacks of Autogenous Bone Grafting
Although the autogenous bone is considered as the gold standard of bone grafting for its osteogenic potential, drawbacks exist which limits its application. Donor site morbidity is of the most concern. Bone harvesting procedures may put adjacent anatomical structures at a risk of damage. For instance during chin bone harvesting, the mental nerve may be pulled under undue traction and the incisive nerve may become interrupted when the harvesting depth is inordinate. Ramal bone harvesting can damage the inferior alveolar nerve.
In addition some patients may be reluctant to the harvesting procedures, especially when extraoral donor sites are concerned. General anesthesia is mandatory for these procedures. Gate problem could occur when autogenous bone is harvested from the tibia or the iliac crest.
2.3 Biomaterials for Guided Bone Regeneration
Guided bone regeneration utilizes the principle concept of guided tissue regeneration which is to separate a space from ingrowth of unintended tissues. Addition of bone graft materials in the space can secure the space from collapsing and promote the speed of bone regeneration. Bioengineering techniques may either enhance osteoinductive properties or mimic osteogenesis in non-autogenous graft materials (Fig. 2.5).
Fig. 2.5
A schematic diagram of the guided bone regeneration technique, (a) Mucoperiosteal flap, (b) GBR membrane, (c) Bone graft material, (d) Host bone bed
2.3.1 Bone Graft Materials
Bone graft materials can be classified according to their source of origin. Each class possesses different capability for regeneration of bone. The most ideal graft material in terms of regeneration potency is the autogenous bone graft which has osteogenetic properties. However application of autogenous bone graft may be restricted. Furthermore, in particular instances of graft material under constant pressure, the autogenous bone graft may fail to secure the graft space. The rapid turnover rate may be problematic. In summary, non-autogenous bone grafts are not simply alternatives to autogenous but may be the best option we have for specific cases.
In Korea, various non-autogenous graft materials are commercially available for clinical use. These allogenic, xenogenic and alloplastic bone graft materials are recommended for small minor bone defects in combination with the guided bone regeneration technique.
2.3.1.1 Allogenic Bone Graft
Allogenic bone graft material originates from human individuals other than the recipient individual, genetically. Bone banks typically accumulate allogenic bone grafts from two donor sources, namely cadaveric and living donors who are undergoing bone removal procedures. Three forms of allogenic bone graft are available. Fresh or fresh-frozen allograft, freeze dried bone allograft and demineralized freeze dried bone allograft. When applying allografts for bone augmentation, the risk of disease transmission is of concern. Fortunately, according to the Centers for Disease Control and Prevention, there have been no reports of disease transmission when freeze-dried types of allograft are used for periodontal procedures.
Advantage of the allogenic grafts over the other bone graft materials is that these grafts can carry osteoinductive properties. Xenogenic and alloplastic bone graft materials are only osteoconductive at the best, unless they are enhanced by bioengineering techniques.
Allogenic bone graft materials available and currently in clinical use in Korea are as in the following. Demineralized freeze-dried form of allografts are Grafton®, Orthoblast II®, Tutoplast®, Regenafil®, and SureFuse®. Freeze-dried bones include Puros®, OraGraft® and ICB®.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


