Oral herpes virus infections (OHVIs) are among the most common mucosal disorders encountered by oral health care providers. These infections can affect individuals at any age, from infants to the elderly, and may cause significant pain and dysfunction. Immunosuppressed patients may be at increased risk for serious and potential life-threatening complications caused by OHVIs. Clinicians may have difficulty in diagnosing these infections because they can mimic other conditions of the oral mucosa. This article provides oral health care providers with clinically relevant information regarding etiopathogenesis, diagnosis, and management of OHVIs.
Key points
- •
Oral herpes virus infections (OHVIs) are commonly encountered in clinical practice.
- •
OHVIs can resemble other types of oral mucosal diseases.
- •
Diagnosis of OHVIs is usually based on patient history and clinical examination findings, but adjunctive laboratory tests may be necessary to establish the diagnosis.
- •
Treatment of OHVIs usually consists of palliative care, but may include use of topical or systemic antiviral medications.
- •
Immunosuppressed patients with OHVIs are potentially at risk of developing life-threatening complications and may require aggressive treatment.
Introduction
There are 80 known herpes viruses, and at least 8 of them are known to cause infections in humans. These viruses include herpes simplex virus (HSV) -1 and -2, varicella – zoster virus (VZV) [human herpes virus {HHV} 3], Epstein – Barr virus (EBV) [HHV-4], Cytomegalovirus (CMV) [HHV-5], HHV-6, -7, and -8 [Kaposi’s sarcoma herpes virus {KSHV}]. There are structural and behavioral characteristics that are common to the members of the herpes virus family (ie, they contain 4 layers: an inner core of double-stranded DNA, a protein capsid, the tegument, and a lipid envelope containing glycoproteins derived from the nuclear membrane of host cells). Herpes viruses cause a primary infection when the person initially contacts the virus, and it remains latent within the nuclei of specific cells for the life of the individual. The site of latency differs among the herpes viruses, with HSV-1, HSV-2, and VZV remaining latent in the sensory nerve ganglia; EBV in B lymphocytes, oropharyngeal epithelial cells, and salivary gland tissue ; CMV in monocytes, bone marrow hematopoietic progenitor cells, epithelial cells, endothelial cells, and possibly, salivary gland tissue ; and HHV-6 and HHV-7 in CD4 lymphocytes. HHV-8 also remains latent in B lymphocytes circulating in the hematopoietic system. After reactivation, herpes viruses can cause localized or disseminated recurrent infections. They are transmitted between hosts by direct contact with saliva or genital secretions. HHV-8 may be transmitted via organ transplantation. Viruses are often shed in the saliva of asymptomatic hosts, who act as vectors for new primary infections in previously non-infected individuals. EBV has been associated with malignancies in humans, such as nasopharyngeal carcinoma and B-cell lymphomas. Other malignancies are associated with EBV, including nasal T-cell/natural killer cell lymphoma seen most commonly in Southeast Asia. HHV-8 has been definitively linked to malignant processes, such as KS, as well as several lymphoproliferative disorders and Castleman disease.
Introduction
There are 80 known herpes viruses, and at least 8 of them are known to cause infections in humans. These viruses include herpes simplex virus (HSV) -1 and -2, varicella – zoster virus (VZV) [human herpes virus {HHV} 3], Epstein – Barr virus (EBV) [HHV-4], Cytomegalovirus (CMV) [HHV-5], HHV-6, -7, and -8 [Kaposi’s sarcoma herpes virus {KSHV}]. There are structural and behavioral characteristics that are common to the members of the herpes virus family (ie, they contain 4 layers: an inner core of double-stranded DNA, a protein capsid, the tegument, and a lipid envelope containing glycoproteins derived from the nuclear membrane of host cells). Herpes viruses cause a primary infection when the person initially contacts the virus, and it remains latent within the nuclei of specific cells for the life of the individual. The site of latency differs among the herpes viruses, with HSV-1, HSV-2, and VZV remaining latent in the sensory nerve ganglia; EBV in B lymphocytes, oropharyngeal epithelial cells, and salivary gland tissue ; CMV in monocytes, bone marrow hematopoietic progenitor cells, epithelial cells, endothelial cells, and possibly, salivary gland tissue ; and HHV-6 and HHV-7 in CD4 lymphocytes. HHV-8 also remains latent in B lymphocytes circulating in the hematopoietic system. After reactivation, herpes viruses can cause localized or disseminated recurrent infections. They are transmitted between hosts by direct contact with saliva or genital secretions. HHV-8 may be transmitted via organ transplantation. Viruses are often shed in the saliva of asymptomatic hosts, who act as vectors for new primary infections in previously non-infected individuals. EBV has been associated with malignancies in humans, such as nasopharyngeal carcinoma and B-cell lymphomas. Other malignancies are associated with EBV, including nasal T-cell/natural killer cell lymphoma seen most commonly in Southeast Asia. HHV-8 has been definitively linked to malignant processes, such as KS, as well as several lymphoproliferative disorders and Castleman disease.
HSV
HSV-1 and HSV-2 are the two major types of herpes viruses known to cause most common oral and perioral infections. They can be distinguished by the distinct antibodies that are formed against each type of virus or by analysis of the nuclear DNA by restriction endonuclease analysis. Classically, HSV-1 causes most cases of oral and pharyngeal infection, meningoencephalitis, and dermatitis above the waist; HSV-2 is implicated in most genital and anal infections. Depending on sexual practices, both types can cause primary or recurrent infections in the oral, perioral, or genital area. HSV infections of the finger (herpetic whitlow) develop after contact with infected saliva or bronchial secretions. The incidence of herpetic whitlow is 4 cases per 100,000 per year.
Primary herpes simplex infections
The incidence of primary infections with HSV-1 increases after 6 months of age as a result of loss of anti-HSV antibodies acquired from the mother during gestation. The incidence of primary HSV-1 infection reaches a peak between 2 and 3 years of age. Primary HSV-1 infections may still occur in adolescents and adults, with occasional cases being reported in patients older than 60 years. Incidence of primary HSV-2 infection does not increase until sexual activity begins. In a prevalence study between 1999 and 2004, 57.7% of the US population tested had HSV-1 antibodies. Data from the Centers for Disease Control showed that 16.2% of Americans aged between 14 and 49 years had HSV-2 antibodies. This prevalence was higher among women (20.9%) compared with men (11.5%) and higher among Blacks (39.2%) compared with Whites (12.3%).
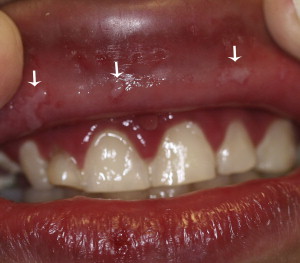
Many primary herpes infections are subclinical or cause pharyngitis, which is difficult to distinguish from other upper respiratory viral infections. Symptomatic primary HSV disease is preceded or accompanied by systemic symptoms, which may include fever, headache, malaise, nausea, vomiting, and accompanying lymphadenopathy. These prodromal symptoms are important to consider when clinically differentiating HSV infections from other vesiculoulcerative diseases of the oral cavity. In the oral cavity, vesicles and ulcers appear on the oral mucosa and generalized acute marginal gingivitis occurs 1 to 2 days after the prodromal symptoms appear ( Fig. 1 ). Primary HSV in healthy children is a usually a self-limiting disease, with fever disappearing in 3 or 4 days and oral lesions that heal in a week to 10 days.
Treatment of primary HSV infection is usually palliative. Milder cases can be managed by supportive care, including maintenance of fluids, use of acetaminophen to reduce fever, and use of topical anesthetics such as viscous lidocaine or a mixture of liquid benadryl, milk of magnesia, and carafate to decrease oral pain. If the patient presents to the clinician within 24 to 48 hours of onset of vesicle eruption, antiviral medication may be helpful to accelerate healing time of the lesions by inhibiting DNA replication in HSV-infected cells. Acyclovir, an antiviral medication, has been shown to decrease symptoms of primary HSV infection in children, including days with fever and viral shedding. Valacyclovir and famciclovir are also common antiviral agents used to treat primary HSV infections; because of their increased bioavailability compared with acyclovir, treatment is effective with fewer daily doses ( Table 1 ).
| Acyclovir | Valacyclovir | Famciclovir | ||
|---|---|---|---|---|
| Dose (mg) | 200 a | 400 b | 1000 a | 250 b |
| Frequency (x/d) | 5 | 3 | 2 | 3 |
| Duration (d) | 7–10 | 7–10 | 7–10 | 7–10 |
a US Food and Drug Administration treatment recommendations for genital herpes.
b Recommendations from the Centers for Disease Control and Prevention for genital herpes.
Recurrent herpes simplex infection
After resolution of a primary HSV infection, the virus migrates to the trigeminal nerve ganglion, where it is capable of remaining in a latent state. Reactivation of virus may follow exposure to cold, exposure to sunlight, stress, trauma, or immunosuppression and cause recurrent infection. Recurrent herpes labialis (RHL) is the most common form of recurrent HSV infection, typically appearing on the mucocutaneous junction of the lip, and is often referred to as a cold sore or fever blister ( Fig. 2 ). Recurrent herpes infections in healthy patients should be treated on a symptomatic basis. Treatment, as well as chronic suppression, of severe, painful, or deforming recurrent herpes may require systemic antiviral medications.

Studies comparing topical antiviral medications for treating RHL have been published. Topical penciclovir reduces the duration and pain of RHL by 1 to 2 days. The recommended dosage of topical penciclovir is application to the area every 2 hours for 4 days while awake. Acyclovir is also available for topical use and has been reported to decrease duration of RHL lesions by 12 hours. Studies have investigated the use of 10% n-docosanol cream and found that when applied 5 times a day for 10 days, it significantly accelerates healing time and decreases pain, especially if commenced during the prodrome. The US Food and Drug Administration has approved n-docosanol as the only non-prescription medication for treatment of RHL. Overall, the benefit of applying these medications to RHL lesions is limited compared with topical penciclovir. Some clinicians advocate the off-label use of suppressive doses of systemic antivirals to prevent severe, frequent disfiguring recurrences of RHL in immunocompetent patients.
Although most recurrent herpes infections occur on the lips and heavily keratinized mucosa of the palate and gingiva, recurrent intraoral herpes (RIH) can occur on any intraoral mucosal surface and is seen more frequently in immunocompromised patients ( Fig. 3 ). Patients at high risk for severe recurrences are those receiving cancer chemotherapy or immunosuppressive drugs to prevent graft rejection after transplantation, as well as patients with advanced AIDS. Recurrent HSV lesions in immunocompromised patients appear as progressively enlarging ulcers, which may involve large portions of the labial, intraoral, genital, or rectal mucosa if left untreated. These lesions have the potential to disseminate and cause generalized infection ( Fig. 4 ); therefore, it is imperative for clinicians to rule out HSV as a cause of oral vesicles or ulcers in immunosuppressed individuals.


Immunosuppressed patients with HSV infection generally respond well to acyclovir administered orally or intravenously. Cases of acyclovir-resistant HSV have been reported, and foscarnet, another antiviral drug, has been effective therapy for these patients. Valacyclovir should be used with caution for immunosuppressed patients, because of the potential risk of hemolytic uremic syndrome. A comprehensive listing of medications and recommended dosing regimens used to treat recurrent oral HSV infections are given in Table 2 .
| Indication | Therapy |
|---|---|
| Treatment of RHL in the immunocompetent host |
|
| Prophylaxis of RHL in the immunocompetent host a |
|
| Treatment of recurrent HSV infections in the immunocompromised host |
|
| Prophylaxis of recurrent HSV infections in the immunocompromised host |
|
a Duration of the prophylaxis is based on the extent and frequency of exposure to triggers of RHL episodes, such as sunlight, dental treatment, and so forth.
Recurrent HSV has been known to trigger episodes of erythema multiforme (EM). HSV is believed to be the most common cause of recurring episodes of EM in susceptible individuals who develop an immune response to HSV. Patients who experience severe, recurring EM from HSV commonly receive prophylactic doses of antiviral medication to prevent recurrence of EM. Oral acyclovir 400 mg twice daily may be effective in suppressing EM, and in cases non-responsive to acyclovir, valacyclovir 500 mg twice daily may be used.
Diagnosis
Differential Diagnosis
Most HSV infections are diagnosed clinically; however, a differential diagnosis should be formulated that includes other vesiculoulcerative diseases. Recurrent aphthous stomatitis (RAS) is commonly misdiagnosed as an HSV infection; however, there are key clinical features that are unique to each disease. HSV infections typically have a prodrome of systemic symptoms before vesicle/ulcer eruption; RAS generally does not have the same prodromal symptoms before ulcer formation. HSV infections usually present with associated gingival erythema; this is uncommon with RAS.
HSV infections may appear clinically similar to coxsackie viral infections, the most common being herpangina and hand-foot-and-mouth disease. Herpangina can be differentiated from HSV infection because lesions associated with herpangina are typically confined to the posterior oropharynx, including the soft palate, uvula, tonsils, and pharyngeal wall. In contrast, HSV lesions may appear throughout the oral cavity. Herpangina infections are usually milder than HSV infections, generally occur in epidemics, and do not cause a generalized acute gingivitis seen with primary HSV infection. Hand-foot-and-mouth disease can also present with oral ulcerations and can be differentiated from HSV infection by lesions involving the hands and feet.
EM may also be considered in the differential diagnosis of HSV infections. Distinguishing features of an EM infection include intraoral lesions, with a wide range of clinical presentations and typically associated target lesions on the skin. In contrast, HSV lesions tend to be more uniform and consistent in clinical presentation. In addition, EM lesions do not typically appear on the gingival tissue or cause gingival erythema, which are characteristic features of HSV infections.
Laboratory Diagnosis
Laboratory tests may be necessary to diagnose atypical presentations of HSV infections. These tests should be used when evaluating immunocompromised patients with atypical lesions for definitive diagnosis.
Virologic tests
The classic standard for virus identification and diagnosis is isolation in tissue culture. The goal of virus isolation is to observe cytopathic effects (CPE) of the cells inoculated with virus. CPE are the degenerative changes that cells undergo when infected with virus. The rate at which CPE develops is dependent on the type of host cell, the type of virus, and the concentration of virus. When viewed at high power via light microscopy, virally infected cells show multinucleated giant cells, syncytium, and ballooning degeneration of nuclei.
Cytology smears
A smear taken of epithelial cells at the base of a suspected lesion may be analyzed to determine if these cells show changes consistent with HSV infection. The most common stain used is Giemsa, and virally infected cells have the same characteristics that are shown by virologic testing. When a Papanicolaou stain is performed, eosinophilic intranuclear viral inclusion bodies (Lipschutz or Cowdry type A) can be seen.
Immunomorphologic tests
The diagnosis of herpes virus infections can be made more quickly and accurately by using immunomorphologic techniques. In the direct fluorescent assay (DFA), the specimen is incubated with fluorescein isothiocyanate–labeled HSV type-specific monoclonal antibody. The positively infected cells are fluorescent green when examined under a fluorescent microscope, and this technique is often used for the rapid diagnosis of a clinical specimen. Studies have concluded that the overall sensitivity when using DFA techniques to detect HSV is 80%, the specificity is 98% to 100%, and the positive predictive value ranges from 90% to 100%.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


