In this case report, we present an unusual approach that was used to treat a 14-year-old patient with a bilateral canine-premolar transposition and a missing maxillary lateral incisor. The orthodontic treatment involved maintaining the transposition and creating a space for lateral incisor replacement. Toward the end of the treatment, accentuated buccal root torque was performed, and lateral group function was established to improve the treatment outcome. Finally, an ideal esthetic and functional occlusion was achieved. The 8-year posttreatment follow-up records show the stability of this treatment.
Tooth transposition is a relatively rare condition in which a permanent tooth develops and erupts in a position normally occupied by another permanent tooth. Maxillary canine-premolar transposition is the most frequent type of tooth transposition, and several theories have been proposed to explain this condition. Genetic origin, prolonged retention of deciduous teeth, supernumerary teeth, and local pathologic processes are some reported causes.
Transpositions in the mixed dentition are usually corrected when the dentoalveolar process has adequate width, the canine involved in the transposition has not completely erupted, and the transposition is not yet completed. However, when the teeth involved have fully erupted and are almost aligned, and the dentoalveolar process is narrow, a satisfactory result can be obtained by maintaining the trans-posed teeth, preventing root resorption and gingival recession, and avoiding prolonged orthodontic treatment.
Here, we present a patient with bilateral maxillary canine-premolar transposition and a missing maxillary lateral incisor, who was treated by maintaining the transposed tooth positions with particular attention to function and esthetics. We also present the long-term follow-up findings.
Diagnosis and etiology
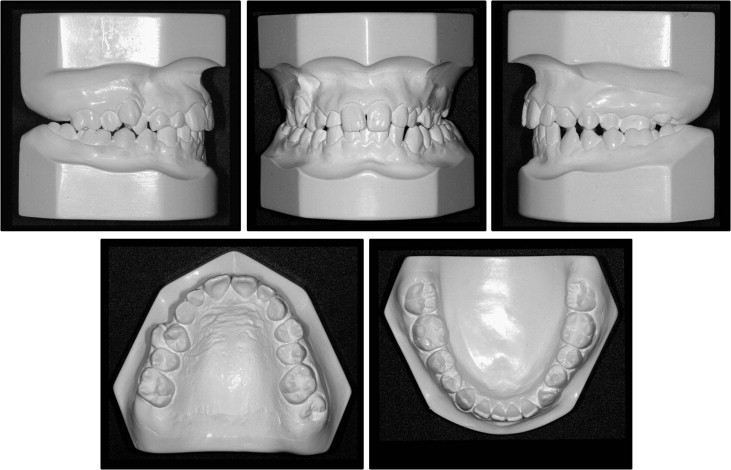
A healthy 14-year-old girl came to us with her parents for the treatment of crowding of the teeth in both arches and the absent maxillary right permanent lateral incisor and left permanent canine. She had a straight profile and symmetric facial development ( Fig 1 ). The intraoral clinical examination showed an Angle Class II malocclusion with left subdivision. We observed prolonged retention of both maxillary deciduous canines, absence of the right lateral incisor, and complete transposition of the right permanent canine with the first premolar. In addition, a unilateral posterior crossbite on the left side was observed ( Fig 2 ).

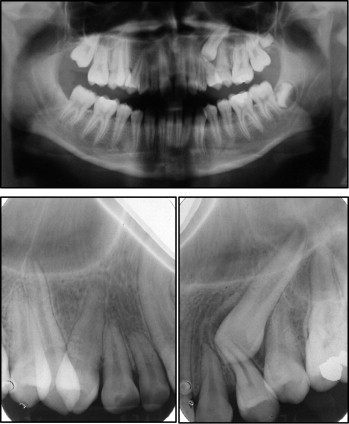
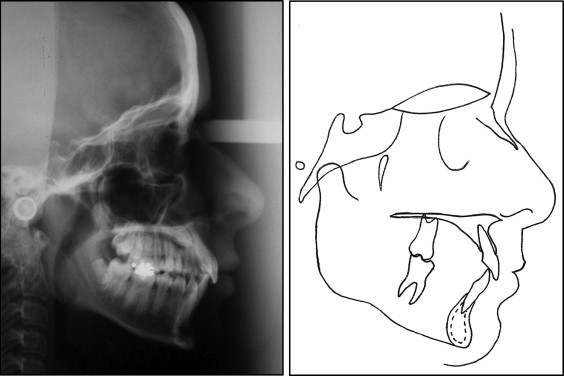
The radiographic examination showed complete transposition on the right side and impaction of the maxillary left permanent canine with accentuated mesial inclination and incomplete transposition with the first premolar. Moreover, the absence of the maxillary right lateral incisor was confirmed ( Fig 3 ). Cephalometrically, she had a good facial pattern with the mandibular incisors in a good position and the maxillary incisors slightly retroclined ( Fig 4 ; Table ).
| Measurement | Norm | Pretreatment ∗ | Posttreatment † |
|---|---|---|---|
| SNA (°) | 82 | 83 | 81 |
| SNB (°) | 80 | 78 | 78 |
| ANB (°) | 2 | 5 | 3 |
| Mx1.NA (°) | 22 | 19 | 24 |
| Mx1-NA (mm) | 5 | 5 | 6 |
| Md1.NB (°) | 25 | 25 | 24 |
| Md1-NB (mm) | 5 | 7 | 6 |
| Mx1.Md1 (°) | 131 | 133 | 130 |
| SN.GoGn (°) | 32 | 29 | 29 |
| FMA (°) | 25 | 21 | 22 |
| FMIA (°) | 60 | 62 | 62 |
| IMPA (°) | 95 | 97 | 96 |
| Upper lip-S line (mm) | 0 | 0 | −2 |
| Lower lip-S line (mm) | 0 | 1 | −2 |
Treatment objectives
The treatment objectives for this patient were to (1) correct the posterior crossbite on the left side, (2) establish a Class I molar relationship on the left side, (3) extract the maxillary deciduous teeth, (4) maintain the maxillary canine-premolar transposition on the right side and perform a prosthetic replacement of the permanent lateral incisor, (5) move the impacted canine on the left side while maintaining the transposition, and (6) establish ideal overbite, overjet, and adequate occlusion with group function in lateral excursion.
Treatment objectives
The treatment objectives for this patient were to (1) correct the posterior crossbite on the left side, (2) establish a Class I molar relationship on the left side, (3) extract the maxillary deciduous teeth, (4) maintain the maxillary canine-premolar transposition on the right side and perform a prosthetic replacement of the permanent lateral incisor, (5) move the impacted canine on the left side while maintaining the transposition, and (6) establish ideal overbite, overjet, and adequate occlusion with group function in lateral excursion.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


