Introduction
The aim of this study was to test the null hypothesis that increased irregularity of the mandibular incisors is associated with a reduction in the alveolar support on cone-beam computed tomographic sections.
Methods
From a sample of 1100 digital volumetric tomographs, 125 tomographs of subjects with Class I malocclusion (mean age, 21.6 ± 4.8 years) were selected for this study. An irregularity index was used to categorize these tomographs as having mild, moderate, or severe crowding. All tomographs were taken by using an iCAT (Imaging Sciences International, Hatfield, Pa) imaging device. The following parameters were measured on the sections corresponding to the 4 mandibular incisors with the iCAT software: height, thickness, and area of the entire symphysis; height, thickness, and area of the cancellous bone of the symphysis; and distance between the vestibular and lingual cortices. For the statistical evaluation, independent samples t test, analysis of variance, and the Tukey HSD test were used at an alpha level 0.05. The Pearson correlation coefficient and a simple linear regression were calculated to determine the relationship between mandibular anterior bony support and incisor crowding.
Results
Almost all mandibular anterior bone measurements were greater in the male subjects than in the female subjects (height of the mandibular symphysis, P <0.001; cancellous bone height, P <0.001). Female subjects with mild crowding had higher values for cancellous bone height ( P = 0.025) and vestibular cancellous bone thickness ( P = 0.004) than did those with severe crowding. However, no differences were detected in the male subjects. Additionally, significant correlations were determined between incisor crowding and thickness of the mandibular symphysis, cancellous bone thickness, and the vestibular part of cancellous bone thickness in female subjects.
Conclusions
Significant relationships were found between the measures of mandibular incisor crowding and basal bone dimensions in female subjects. Except for the vestibular part of cancellous bone thickness, all mandibular incisor bone measurements were greater in the male subjects than in the female subjects.
Crowding of the mandibular incisors is a critical issue because it has an impact on prognosis, treatment methods, and retention. Several factors can be assumed to affect the development and severity of crowding, such as the direction of mandibular growth, early loss of the deciduous molars, mesiodistal tooth and arch dimensions, oral and perioral musculature, and incisor and molar inclinations. The attempt to establish an orthodontically ideal, long-lasting, and equilibrated position of the incisors has included the possible determination of the anteriormost limit of the teeth.
The mandibular symphysis is the anatomic factor that limits the movement of the incisors. The small labiolingual dimension of the alveolar process in this area implies a thin layer of bony support of the mandibular incisors. Wehrbein et al suggested that, in the case of a narrow and high symphysis, extensive orthodontic tooth movements during routine orthodontic treatment with a fixed appliance might be critical and lead to progressive bone loss of lingual and labial cortical plates. Fuhrmann has shown that loss of thin bone plates can be induced by orthodontic tooth movement. Therefore, the choice of treatment plan should be greatly influenced by the morphology of the symphysis and the position of the mandibular incisors.
Cone-beam computed tomography (CBCT) has become a popular modality in the evaluation of orthodontic diagnosis and outcomes. CBCT enables us to examine the shape and the size of alveolar bones without the disadvantages of conventional radiographs. Unlike conventional radiographs, there is no magnification and distortion in CBCT images.
Only a few studies have evaluated the mandibular bone with computerized tomography. Gracco et al evaluated mandibular incisor bony support in untreated patients with various facial types via computed volumetric tomography and found a statistically significant relationship between facial type and the total thickness of the mandibular symphysis. Siciliani et al found that the symphysis is thin and elongated in patients with long faces, whereas it is thicker in those with short faces. Tsunori et al established a correlation between facial type and mandibular cortical bone thickness. Yamada et al indicated that the morphology of the alveolar bone in the central incisor region might be associated with the inclination of the central incisors.
Because the teeth and the neighboring bony structures are in a close relationship, a reciprocal effect can occur, and they might be affected by each other. To our knowledge, no research in the literature has investigated the correlation between mandibular bony support and mandibular incisor crowding with CBCT. Thus, the aim of this study was to test the null hypothesis that increased irregularity of the mandibular incisors is associated with a reduction in the alveolar support on CBCT sections.
Material and methods
Before this study, a power analysis with G*Power (version 3.0.10; Franz Faul, Christian-Albrechts-Universität, Kiel, Germany) was performed to estimate the sample size. It showed that a total sample size of 111 subjects would give more than 80% power (actual power, 0.8034; critical F, 3.0803; noncentrality parameter, λ = 9.99), or 126 subjects would give more than 85% power (actual power, 0.8548; critical F, 3.0698; noncentrality parameter, λ = 11.34) to detect significant differences with a 0.30 effect size and at an α = 0.05 significance level.
Permission was obtained from the Dicle University Human Researches Regional Ethical Committee after its Research Scientific Committee had approved the experimental protocol. All CBCT scans were selected from the archive of the university’s Oral and Maxillofacial Radiology department. The CBCTs for these patients had been taken at their usual records appointments as a part of the necessary radiographs; therefore, the subjects were not unnecessarily subjected to additional radiation.
By September 2010, images of 1100 patients (ages, 8.5-67.3 years) were in the database. CBCT scans of subjects with syndromes, craniofacial malformations, evidence of trauma, and periodontal diseases, those who had had orthognathic surgery or previous orthodontic treatment, and those with congenitally missing or extracted permanent teeth (except third molars) were excluded from the initial sample of 1100 digital volumetric tomography scans. From the remaining tomography scans, 125 tomographs of subjects with Class I malocclusion, aged 16 to 36 years (mean age, 21.6 ± 4.8 years), were selected for this study. The subjects with Class II and Class III malocclusions were excluded to eliminate probable compensation mechanisms that might affect the inclination of the mandibular incisors. The selected patients were categorized according to Little’s irregularity index as having mild, moderate, or severe crowding.
All tomographs were obtained with the iCAT imaging device (model 17-19; Imaging Sciences International, Hatfield, Pa) at the following settings: the x-ray emission time was 3.5 seconds, exposures were made at 5.0 mA and 120 kV, exposure time was 9.6 seconds, and axial slice thickness was 0.3 mm. Also, primary and secondary reconstructions of the data were performed with the iCAT software. This secondary reconstruction permitted the creation of 3-dimensional maximum-intensity projection images, from which it was possible to make the linear and angular measurements.
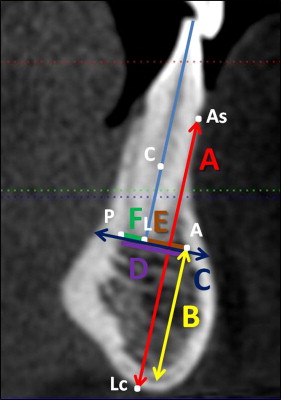
All measurements were performed by using the distance-measuring property of the iCAT software, and the CBCT landmarks were designated by 1 author (I.V.). All landmarks used in this study are given and defined in Table I .
| A point: the point on the internal surface of the anterior cortex |
| P point: the point on the internal surfaces of the posterior cortex |
| As point: the most anterosuperior point of the mandibular alveolar process |
| Lc point: the point formed by the intersection of external surface of the lingual cortex and the line parallel to the axis of the incisors and crossing the As point |
| Center of rotation (C): the midpoint of the incisor root position embedded in alveolar bone |
| L point: the apex of the root |
| CH line: the line parallel to the axis of the incisor from the vestibule to the lingual cortex of the symphysis |
| MT line: the line perpendicular to the axis of the incisor that passes through the apex of the root between the external surfaces of the lingual and vestibular cortices |
| A-P size: the arc between points A and P that corresponds to the cancellous bone thickness of the alveolar process |
| A-L size: the arc between points A and L that identifies the vestibular portion of the cancellous bone of the symphysis |
| L-P size: the arc between points L and P identifies the lingual portion of the cancellous bone of the symphysis |
To examine the osseous variables in the region of the incisors, the following measurements were calculated for all mandibular incisors on the sagittal slices ( Fig 1 ): (1) height of the mandibular symphysis, (2) cancellous bone height of the mandibular symphysis, (3) thickness of the mandibular symphysis, and (4) cancellous bone thickness of the mandibular symphysis. We subsequently divided the cancellous bone thickness into vestibular and lingual portions. The sagittal slices were arranged so that the vertical reference line on the panoramic view passed through the central axis of the incisors. Twenty-four CBCT measurements (6 measurements for the section of each incisor level) were made for each of the 125 patients, giving 3000 measurements.
CBCT scans were also used to evaluate crowding ( Fig 2 ). The irregularity index proposed by Little was used to evaluate mandibular incisor crowding. The scoring method involves measuring the linear displacement of the anatomic contact points of the anterior teeth. The sum of the 5 measurements represents the subject’s irregularity index value.
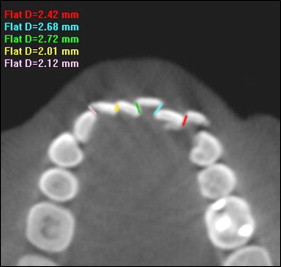
Additionally, to identify possible differences in bony support with different levels of the irregularity index, crowding was classified according to the following criteria: (1) mild, up to 3 mm (spacing was also included); (2) moderate, between 4 and 8 mm; and (3) severe, more than 8 mm.
Statistical analysis
All statistical analyses were performed with the statistical package for social sciences (version 13.0, SPSS for Windows; SPSS, Chicago, Ill). The normality test of Shapiro-Wilks and the Levene variance homogeneity test were applied to the data. The data were normally distributed, and there was homogeneity of variance among the groups. Thus, the statistical evaluation was performed by using parametric tests. Arithmetic mean and standard deviation values were calculated.
To evaluate sex differences in mandibular bony support measurements, the independent samples t test was used. Statistical comparisons of mandibular bone dimensions in subjects with different severities of crowding (mild, moderate, or severe) were undertaken by 1-way analysis of variance (ANOVA) and the Tukey HSD test. To evaluate the correlation between mandibular anterior bony supports and mandibular incisor crowding, Pearson correlation coefficients were estimated, and a simple linear regression analysis was done. When the P value was less than 0.05, the statistical test was determined to be significant.
Results
To determine the errors associated with CBCT measurements, 15 CBCT images were selected randomly. The measurements were repeated 8 weeks later by the same author (I.V.). A Bland-Altman plot was applied to assess the repeatability. The differences between the first and second measurements were not significant.
Comparisons of all bone measurements at the level of the 4 mandibular incisors were made, and no statistically significant differences were found. Thus, the bony support measurements of all incisors were pooled.
Table II summarizes the descriptive statistics and comparisons of sex differences in the mandibular anterior bony support measurements. According to the statistical analysis, only the vestibular part of cancellous bone thickness had no significant sex dimorphism ( P = 0.197). All other measurements showed statistically significant sex differences. All measurements were greater in the male subjects than in the female subjects.
| Measurement (mm) | Female | Male | P value | ||||
|---|---|---|---|---|---|---|---|
| n | Mean | SD | n | Mean | SD | ||
| Height of the mandibular symphysis | 66 | 21.01 | 3.06 | 59 | 23.26 | 2.81 | <0.001 |
| Cancellous bone height | 66 | 11.60 | 2.03 | 59 | 13.27 | 1.99 | <0.001 |
| Thickness of the mandibular symphysis | 66 | 7.79 | 1.80 | 59 | 8.39 | 1.51 | 0.046 |
| Cancellous bone thickness | 66 | 4.92 | 1.38 | 59 | 5.43 | 1.09 | 0.026 |
| Vestibular part of cancellous bone | 66 | 3.29 | 1.15 | 59 | 3.53 | 0.90 | 0.197 |
| Lingual part of cancellous bone | 66 | 1.63 | 0.62 | 59 | 1.89 | 0.56 | 0.015 |
Because there was significant sex dimorphism, the relationship between bone support and mandibular incisor crowding was determined separately for each sex. Statistical comparisons of mandibular anterior bony support in male subjects with different amounts of crowding are shown in Table III . According to the ANOVA, there was no statistically significant difference for the bone measurements among the male subjects with different severities of crowding ( Table III ).
| Measurement (mm) | Mild crowding (0-3 mm) | Moderate crowding (4-8 mm) | Severe crowding (>8 mm) | ANOVA | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | n | Mean | SD | n | Mean | SD | P value | |
| Height of the mandibular symphysis | 24 | 22.86 | 2.76 | 17 | 22.91 | 2.44 | 18 | 24.11 | 3.15 | 0.305 |
| Cancellous bone height | 24 | 12.87 | 1.74 | 17 | 12.94 | 2.23 | 18 | 14.11 | 1.93 | 0.099 |
| Thickness of the mandibular symphysis | 24 | 8.46 | 1.56 | 17 | 8.24 | 1.79 | 18 | 8.45 | 1.22 | 0.889 |
| Cancellous bone thickness | 24 | 5.55 | 1.10 | 17 | 5.15 | 1.27 | 18 | 5.54 | 0.90 | 0.457 |
| Vestibular part of cancellous bone | 24 | 3.51 | 0.86 | 17 | 3.44 | 1.08 | 18 | 3.64 | 0.82 | 0.802 |
| Lingual part of cancellous bone | 24 | 2.02 | 0.65 | 17 | 1.71 | 0.52 | 18 | 1.90 | 0.43 | 0.226 |
However, statistically significant differences were found in 2 of the 6 measurements ( Table IV ) for female subjects. Significant differences were found in cancellous bone height ( P = 0.017) and the vestibular part of the cancellous bone thickness measurements ( P = 0.005). The Tukey HSD analysis indicated that the mild group had higher values for cancellous bone height ( P = 0.025) and the vestibular part of cancellous bone thickness ( P = 0.004) than did the severe group.
| Measurement (mm) | Mild crowding (0-3 mm) | Moderate crowding (4-8 mm) | Severe crowding (>8 mm) | ANOVA | Tukey HSD P value |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mild-moderate | Mild-severe | Moderate-severe | |||||||||||
| n | Mean | SD | n | Mean | SD | n | Mean | SD | P value | ||||
| Height of the mandibular symphysis | 22 | 21.55 | 3.16 | 20 | 20.80 | 2.64 | 24 | 20.68 | 3.33 | 0.596 | |||
| Cancellous bone height | 22 | 12.21 | 2.15 | 20 | 12.05 | 1.78 | 24 | 10.67 | 1.84 | 0.017 | 0.962 | 0.025 ∗ | 0.056 |
| Thickness of the mandibular symphysis | 22 | 8.29 | 1.90 | 20 | 8.04 | 1.48 | 24 | 7.12 | 1.80 | 0.064 | |||
| Cancellous bone thickness | 22 | 5.34 | 1.51 | 20 | 5.03 | 0.86 | 24 | 4.45 | 1.50 | 0.082 | |||
| Vestibular part of cancellous bone | 22 | 3.79 | 1.21 | 20 | 3.40 | 0.80 | 24 | 2.73 | 1.13 | 0.005 | 0.464 | 0.004 † | 0.103 |
| Lingual part of cancellous bone | 22 | 1.55 | 0.67 | 20 | 1.63 | 0.53 | 24 | 1.70 | 0.65 | 0.714 | |||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


