FLORIN LĂZĂRESCU
Chapter VI
ULTRACONSERVATIVE DENTISTRY
Systematic respect for the original tissue, a concept that can be applied to all aspects of dental medicine, is the foundation of ultraconservative dentistry; the common denominator is preservation or minimal removal of dental tissue.
Advanced specialization in various fields of dental medicine (for instance, prosthodontics, periodontics, orthodontics, endodontics, pediatric dentistry, dental implantology, etc) may benefit the patient who enjoys high-quality healthcare. The drawbacks may be a sometimes narrow approach to the case, and lack of perspective in the absence of comprehensive treatment planning, which should take into account the overall health of the patient and the ultraconservative character of the restoration, as well as issues related to pain, mastication, and esthetics.
Patients’ expectations of the healthcare system are completely different today to what they were a few years ago, and are constantly changing due to the ease of access to online information, the growing awareness of general health (regular medical checkups, healthy diets, balanced lifestyles), and patients’ wishes for dental restorations that will last – and have a warranty for – a lifetime. Often, a dentist has to deal with patients who ask for a second or third opinion before they agree on a treatment plan, patients with health issues associated with tooth disorders (temporomandibular joint [TMJ] or muscle disorders, bad habits, etc), or patients with psychological disorders. In many such cases, a highly subjective approach should take priority over objective clinical and paraclinical examinations.1
Taking all the aforementioned aspects into consideration – and considering that people often come to the dentist chiefly to improve their looks – it is extremely important for dentists whose practice is primarily focused on cosmetic dentistry to have a broad and comprehensive overall perspective of the patient’s clinical condition, as well as a multidisciplinary approach to treatment planning. The ultimate purpose is to achieve an ultraconservative and esthetic functional restoration that satisfies the patient, has a long lifespan, and is in agreement with the principles of modern dentistry.
Nowadays, patients are guided by the ultraconservative principle and are reluctant to agree to a treatment plan that does not take this principle into consideration.
6.1.1 Magnification, illumination, and isolation in ultraconservative dentistry
Visibility within the oral cavity is often limited because the dentist’s vision can be restricted by various structures. It can therefore be difficult to access a tight space. In order to gain the best access and visibility inside the oral cavity, the dentist often assumes unnatural and stressful body positions, which in time lead to posture-related musculoskeletal problems and even impaired mobility and working capacity.
The lesser the amount of tooth structure removed during preparation and the smaller the operative site, the greater the amount of equipment needed to assist the dentist in current practice.
Dental magnification loupes and microscopes are really helpful in this respect. The most significant advantages are the following:2
• Visibility is improved.
• Illumination is improved.
• Isolation is controlled.
• Preparation is controlled.
6.1.1.1 Magnification
Dental loupes and microscopes improve ergonomics and ensure that the dentist maintains correct posture, affording more productive and less stressful work sessions, thereby alleviating muscle pain and improving comfort at work (Figs 6-1a and 6-1b).
At the same time, esthetic preparations require precision down to the micron level. One can be certain that a barely visible effect magnified to 2.5 with loupes, or even higher with a microscope, cannot be detected by the human eye.2
While loupes and microscopes were originally used strictly in cosmetic dentistry, they have become indispensable tools in endodontics and periodontics (Figs 6-2a to 6-2d).

Fig 6-1 a Correct body posture of a dental practitioner using loupes.

Fig 6-1 b Correct body posture of a dental practitioner using a microscope.
Whereas loupes were employed by elderly dental practitioners in the past, they are now being used as early as dental school. A survey of 332 dentistry students, 50% of whom used loupes, recorded the number of preparations per time unit and the time required for one preparation. The investigated preparations on dental phantoms comprised class I, II, III, and V cavities. The results were statistically significant in favor of the students who used loupes, both for the number of prepared teeth per time unit and for the cavity preparation speed per procedure for all types of cavities. The study also revealed a high degree of student acceptance of the use of magnification, because in this way they could better self-evaluate their performance.3
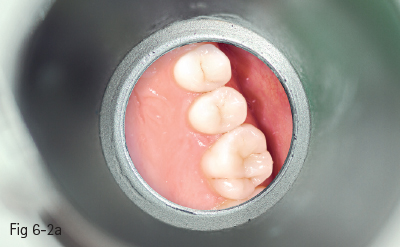
Fig 6-2 a 1:1 ratio visualization of preparation.
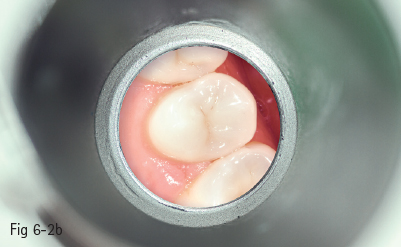
Fig 6-2 b 2.5:1 ratio visualization of preparation with dental loupes.

Fig 6-2 c OPMI pico – ZEISS surgical microscope.
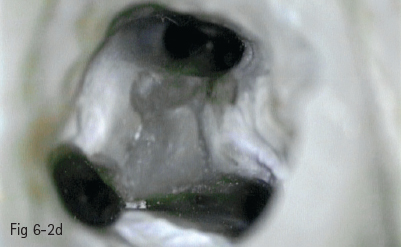
Fig 6-2 d 21:1 ratio visualization of preparation with the optical microscope. (Photo courtesy of Dr Monica Voiculeanu.)

Fig 6-3 a Dental loupes with LED headlight.

Fig 6-3 b Visualization of operative site by means of an external LED source.
Hand in hand with the technological development of dental materials (porcelain, bonding agents, composite resins, and cements) that has made ultraconservative dentistry possible, self-evaluation due to magnification has significantly enhanced performance and the quality of preparations, which has consequently led to better patient satisfaction.
6.1.1.2 Illumination
It is now inconceivable for a dentist to acquire dental equipment without a fiber optic illumination system to light the operating site. However, sometimes a wider visibility area is required. The development of LED technology, and its association with dental loupes by direct attachment to glasses without special support systems, has led to it becoming extremely popular in dental practice (Figs 6-3a and 6-3b).
6.1.1.3 Isolation
During dental procedures, teeth or soft tissues are sometimes not visible enough. Apart from the presence of saliva, the tongue or cheeks may obstruct the operative field. The four-handed technique is quite useful when dealing with this problem.
Yet again, technology has provided helpful tools: for instance, the Isolite isolating system, which consists of a single-use flexible mouthpiece that can be inserted into the oral cavity and is bitten down on by the patient. The system allows the patient to feel relatively comfortable, even during a lengthy treatment. The operative field is illuminated by an LED source. Aspiration is possible both in the oral and facial sides of the field (Fig 6-4).2

Fig 6-4 Isolite system. (Courtesy of Isolite Systems – http://www.isolitesystems.com.)

Fig 6-5 Rubber dam isolation of the operative field for cementation of eight porcelain veneers.

Fig 6-6 a Initial clinical situation.

Fig 6-6 b Change in shape and position by using six porcelain laminate veneers applied from 13 to 23.
The rubber dam is a must for bonding, as it is the only method of isolating teeth that is comfortable for the patient and has a predictable result over a period of time (Fig 6-5).
6.1.2 Preparation in ultraconservative dentistry
In the eyes of both the dentist and the patient, porcelain laminate veneers stand for ultraconservative or minimally invasive dentistry. Dentists and patients alike choose veneers over traditional crowns because they enable a more esthetic restorative procedure. They are also minimally invasive and have a lower risk of subsequent complications. However, if proper tooth preparation is not followed, or treatment planning is incorrect, the restoration may fail.
Porcelain laminate veneers can effect changes in the color, shape, and position of the teeth (Figs 6-6a and 6-6b). In order to avoid any risk, tooth preparation should always be limited to the enamel. On average, considering the initial tooth color and the type of porcelain, dental preparation should go no deeper than 0.4 to 0.8 mm.1
Taking into account the progress achieved in increasing the strength of bonding agents and porcelain, tooth preparation for all-ceramic crowns may be approached as a preparation for an extended veneer. It requires a minimally invasive preparation of all sides of the tooth without strictly following the rules of minimal tooth reduction – such as for porcelain fused to metal (PFM) crowns, for instance. Preservation of the dental structure and the enamel is paramount for this type of preparation.4
Sometimes in clinical situations, the preparation might extend to limited areas of the dentin, chiefly to the cementoenamel junction (CEJ), where the enamel is less thick (Figs 6-7a and 6-7b). Even in the case of the latest adhesives that create a solid and stable bond with the tooth enamel and dentin (in contrast with the first generations of bonding agents that adhered only to the enamel), the adhesion to the enamel is much stronger than it is to the dentin. Therefore, it is recommended that the preparation be limited to the enamel.

Fig 6-7 a Dental preparation limited to the enamel.

Fig 6-7 b Dentin exposure at the cervical part of 13, irrespective of the minimally invasive tooth preparation.


Fig 6-8 a,b Orthodontic alignment in order to permit minimally invasive procedures for tooth preparation.


Fig 6-8 c,d Result after orthodontic alignment.

Fig 6-8 e Maxillary incisors are not visible when the lips are at rest.

Fig 6-8 f Provisional restorations in the oral cavity before preparation (mock-up) according to the wax-up prepared in the dental technical laboratory.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


