The aim of this article is to describe the surgical, orthodontic, and periodontal treatment of an adult patient with a lateral open bite, anterior crowding, and gingival recession on the mandibular right lateral incisor. The lateral open bite, which resisted conventional mechanics, was successfully corrected by the combination of dento-osseous osteotomies and vertical alveolar distraction using orthodontic multibracket appliances in conjunction with nickel-titanium archwires and intermaxillary elastics. After the orthodontic treatment, the denuded root surface of the mandibular right lateral incisor was closed using a coronally advanced flap technique with platelet-rich fibrin. The results at the 2-year posttreatment follow-up were satisfactory from both the occlusal and the periodontal standpoints.
Highlights
- •
Open bite persistent to conventional mechanics was treated by vertical distraction.
- •
Distraction of dento-osseous blocks was achieved by Ni-Ti arch wires and elastics.
- •
Less treatment time and no periodontal complications are the advantages of this method.
A lateral open bite that causes functional and esthetic problems is characterized by infrapositioned teeth below the occlusal plane and vertical underdevelopment of the dentoalveolar processes in the posterior segments. This malocclusion can result from ankylosed teeth, mechanical interference with eruption such as tongue thrust, or a disturbance of the eruption mechanism (primary failure of eruption). The conventional treatment of a lateral open bite involving nonankylosed teeth comprises fixed appliances and intermaxillary elastics to obtain dentoalveoler extrusion in the open-bite region.
Cell mobilization, fibrous tissue reaction, and turnover rate of collagen molecules are slower in adults than adolescents, and bones are denser in adults. These factors result in a delayed onset of responses to mechanical forces and increase the potential for complications such as alveolar bone dehiscence, marginal bone loss, gingival recession, and root resorption in orthodontic treatments of adults, especially when applied to patients with a thin periodontal biotype or when heavy orthodontic forces are used. One way to remove some of the limitations encountered in tooth movement and to simplify the orthodontic treatment and minimize the risk of side effects is distraction osteogenesis. Case reports have shown that vertical continuation of dentulous or edentulous alveolar processes, extrusion of the ankylosed maxillary central incisors, and correction of lateral open bites caused by vertical canting of the lesser segment in cleft palate patients can be achieved with vertical distraction osteogenesis.
This article describes an orthodontic treatment combined with distraction osteogenesis using multibracket appliances in conjunction with nickel-titanium archwires and intermaxillary elastics in an adult patient after traditional orthodontic therapy proved to be ineffective for lateral open-bite correction and describes the periodontal treatment of gingival recession on the mandibular lateral incisor.
Diagnosis and etiology
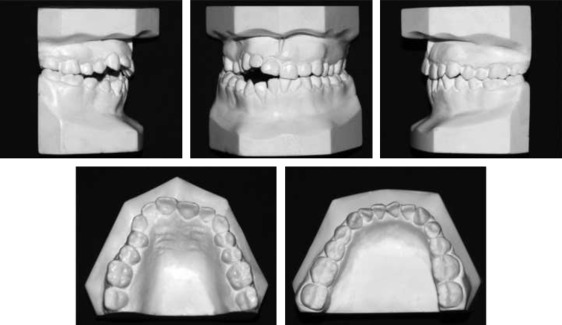
The patient was a 23-year-old white woman with the complaint of a lateral open bite. The extraoral frontal examination showed no asymmetry. Her forced smile disclosed a unilateral open bite in the right buccal and anterior regions, and she had an acceptable gingival display. She had a straight profile with unstrained lip closure. We observed that the tongue was interposed between the teeth on the right side, causing incomplete vertical eruption of the dentition. The patient recalled no history of trauma and showed no signs of temporomandibular joint dysfunction. Her dental history consisted of many amalgam fillings. She had not sought orthodontic treatment before. She had poor oral hygiene and gingival recession on the mandibular right lateral incisor because of a thin labial biotype and inadequate oral hygiene. The intraoral and dental cast examinations in the sagittal direction showed Class I molar relationships on both sides and at the left canines, with a Class II relationship for the right canines. Overjet was 1.5 mm. There was a mild crossbite in the right premolar region with no other buccal crossbite or scissors-bite, and the maxillary and mandibular midlines were coincident with each other and with the facial midline. Vertically, she had an open bite extending from the right first molar to the right central incisor with a peak value of 6.5 mm at the lateral incisor region, and a 4-mm opening at the canine-first premolar region. The cast analysis showed space discrepancies of 3.5 mm in the maxillary arch and 4.2 mm in the mandibular arch ( Figs 1 and 2 ).

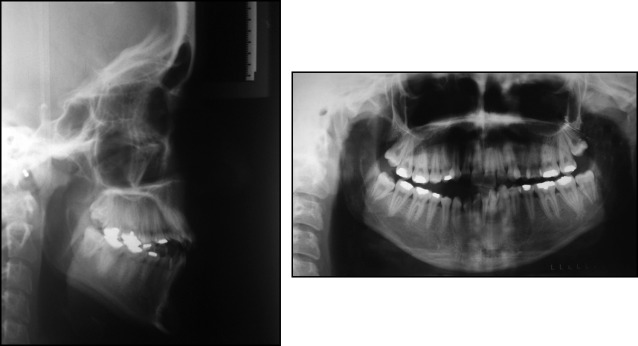
The lateral cephalometric analysis showed a skeletal Class III relationship (ANB, −1.9°; Wits appraisal, −6 mm) with bimaxillary retrognathism relative to the frontal cranial base (SNA, 71.6°; SNB, 73.5°). The patient had a hyperdivergent skeletal pattern (SNGoGn, 44.9°). Although the inclination of the maxillary incisors was normal (1-SN, 102.5°), the mandibular incisors were retroclined (IMPA, 80°). She had a straight profile with retruded upper and lower lips (lower lip to the S-line, −3 mm; upper lip to the S-line, −5.5 mm). All third molars were impacted ( Fig 3 ; Table ).
| Pretreatment | Posttreatment | Two years posttreatment | |
|---|---|---|---|
| SNA (°) | 71.6 | 71.5 | 71.5 |
| SNB (°) | 73.5 | 73.3 | 73.4 |
| ANB (°) | −1.9 | −1.8 | −1.9 |
| Wits (mm) | −6.0 | −3.8 | −3.7 |
| SNGoGn (°) | 44.9 | 44.5 | 44.3 |
| U1-SN (°) | 102.5 | 106.3 | 106.6 |
| IMPA (°) | 80.0 | 87.8 | 87.8 |
| Upper lip-S line (mm) | −5.5 | −4.1 | −4.0 |
| Lower lip-S line (mm) | −3.0 | −2.2 | −2.2 |
No history of trauma was recalled. Also, the possibility of primary failure of eruption was ruled out because the anomaly did not include the molars. Although the vertical skeletal dimensions were increased, because there was dentoalveolar compensation on the left since we postulated that the orofacial dysfunction (tongue thrust) was the main etiologic reason for this regional open bite.
Treatment objectives
The main treatment objectives were to (1) correct the unilateral open bite by extrusion of the maxillary and mandibular teeth, (2) resolve the maxillary and mandibular crowding, (3) obtain Class I molar and canine relationships with normal overjet, overbite, and symmetrical dental arches, (4) improve the periodontal conditions of the mandibular right lateral incisor, and (5) achieve stable treatment results.
Treatment objectives
The main treatment objectives were to (1) correct the unilateral open bite by extrusion of the maxillary and mandibular teeth, (2) resolve the maxillary and mandibular crowding, (3) obtain Class I molar and canine relationships with normal overjet, overbite, and symmetrical dental arches, (4) improve the periodontal conditions of the mandibular right lateral incisor, and (5) achieve stable treatment results.
Treatment alternatives
The primary treatment option to achieve dentoalveolar extrusion was to use conventional orthodontics, including a multibracket system and intermaxillary elastics. Other options would be immediate repositioning of the teeth with segmental osteotomies and corticotomy-assisted orthodontic treatment. Also, surgical osteotomies followed by distraction osteogenesis to overcome the various shortcomings of conventional orthodontic treatment, such as the long treatment time and the limited amount of tooth movement, could be efficient alternatives.
Treatment progress
Before commencement of the orthodontic treatment, the patient was advised to consult a periodontist because of her poor overall oral hygiene and gingival recession on the mandibular right lateral incisor. Full-mouth scaling was performed by the periodontist. Periodontal surgery to cover the root was recommended after active orthodontic treatment because there is a risk of recurrence of gingival recession during treatment as the tooth is being moved; additionally, a well-positioned tooth will simplify the achievement of a correct gingival contour. Moreover, the patient was referred to the oral surgeon for removal of the mandibular right third molar to aid in the uprighting of the first molar. We placed 0.018-in preadjusted edgewise appliances simultaneously in both arches, and 0.012-in, 0.014-in, and 0.016-in nickel-titanium archwires were used for leveling and aligning. Additionally, the patient was instructed to use 100-g intermaxillary elastics from the palatal buttons on the maxillary right premolars to the buccal hooks on the mandibular right premolars; the elastics also acted as a barrier to the tongue thrust. Although the maxillary teeth were almost leveled and aligned by 6 months after the start of treatment, no leveling was achieved at the right segment of the mandibular arch extending from the second premolar to the canine ( Fig 4 ). It was postulated that the more compact structure of the mandibular bone compared with the maxilla together with the interference by the tongue thrust resisted the efforts to extrude the posterior teeth when light forces were used. The other possibility was ankylosis of the mandibular right canine and premolars. When confronted with these possibilities, we planned to move the teeth with the supporting bone via osteotomies followed by distraction osteogenesis.

Surgical procedure
Mandibular unitooth and segmental osteotomies were performed using a Lindermann single-piece carbide bur (Dental Burs USA, Napa, CA) after a mucoperiosteal flap was reflected under local anesthesia. Vertical cuts were made on both the mesial and distal interproximal areas of the teeth in the mandibular right quadrant starting from the first molar and ending at the distal aspect of the right canine, beginning 2 to 3 mm below the alveolar crest and extending 3 mm beyond the estimated root apex. Additionally, a segmental osteotomy ending at the mesial aspect of the left canine with a vertical cut was incorporated at the incisors. Then a buccal horizontal cut was made 3 mm below the root apices connecting the vertical cuts and extending from the distal aspect of the right first molar to the mesial aspect of the left canine. These cuts were made as deep as possible into the bone from the labial side. Hence, single-tooth osteotomies consisting of the mandibular right first molar and the second and first premolars, as well as a segmental osteotomy comprising the right canine and incisors were done ( Fig 5 ). During the osteotomies, great care was taken not to injure the lingual periosteum and mucosa. The alveolar segments were mobilized with an osteotome. The mucoperiosteal flap was then closed without repositioning the mobilized segments.

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


