An 8-mm anterior and posterior open bite caused by a tongue rest posture habit was closed in a 25-year-old man by means of mandibular soldered tongue spurs and without orthognathic surgery. All maxillary and mandibular first molars were extracted, and the spaces were closed. Inappropriate retention protocol allowed for relapse in a 6-month period. A new 1-year orthodontic retreatment was conducted; after an appropriate retention protocol, the outcomes of treatment were significantly improved.
Open-bite patients with anterior tongue rest posture or thrust problems have been treated with many different therapies. Some examples are vertical elastics, orthognathic surgery, tongue cribs, tongue spurs, multiloop edgewise archwires, and temporary anchorage devices. However, it has been documented that relapse of the corrected open bite frequently occurs and is therefore a major concern.
Improper tongue rest posture has been suggested as the primary contributing factor to anterior open bites. Justus demonstrated that anterior open bites can be safely and effectively closed using soldered tongue spurs to a maxillary lingual arch, and that the results remain stable because of the triggering of a nociceptive or proprioceptive reflex to prevent soreness; this results in a new engram. However, additional possible etiologies can cause anterior open bites, including vertical growth deficiencies and thumb and lip sucking habits.
A review of the scientific literature showed that anterior tongue rest posture is a primary contributing factor to anterior open bite, that the use of tongue spurs does correct an anterior open bite by modifying anterior tongue posture, and that long-term stability is achieved because a new tongue posture engram is established. Prevention of anterior open-bite relapse by using tongue spurs during orthodontic treatment to modify anterior tongue posture has been substantiated in numerous studies. The uniqueness of this case report lies in the fact that a significant open bite was closed simply by modifying an anterior tongue rest posture with tongue spurs and without the need for orthognathic surgery.
This patient presented 3 challenges: a severe open-bite malocclusion, 4 first molar spaces to be closed, and the need for a proper retention protocol to prevent relapse. De Freitas et al reported that in a sample that required extraction of 4 premolars, the greater the treatment changes needed and the smaller the posttreatment peer assessment rating score, the greater the relapse. O’Neill, in a systematic review of long-term stability after orthodontic treatment, reported that despite many studies, evidence-based conclusions about retention are few. The lack of agreement on a retention protocol might have contributed to the wrong retention approach in this patient, who required retreatment.
Diagnosis and etiology
A 25-year-old man was referred to the orthodontic office of the first author in Curitiba, Brazil, by his periodontist because he “could not close with his front teeth, and his first molars were significantly loose.” He did not report any medical problems and was not taking any medication. The periodontist had initiated treatment 1 year earlier and had performed deep root scaling associated with periodontal flap surgery in an attempt to save the mandibular first and second molars.
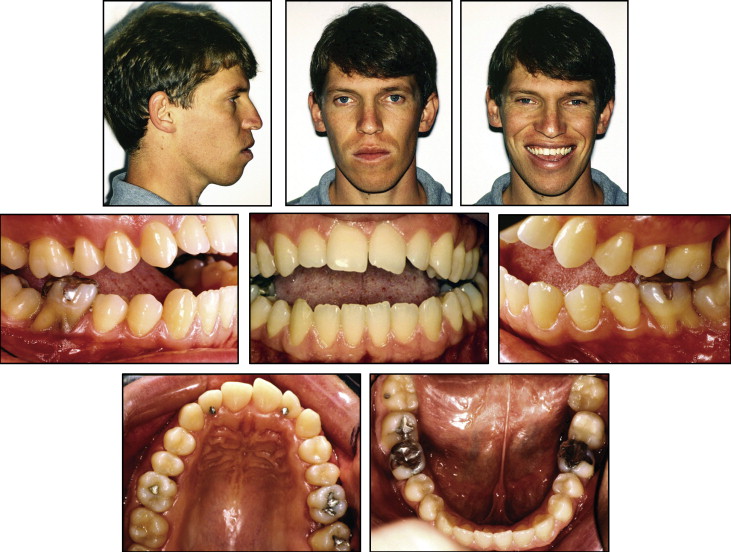
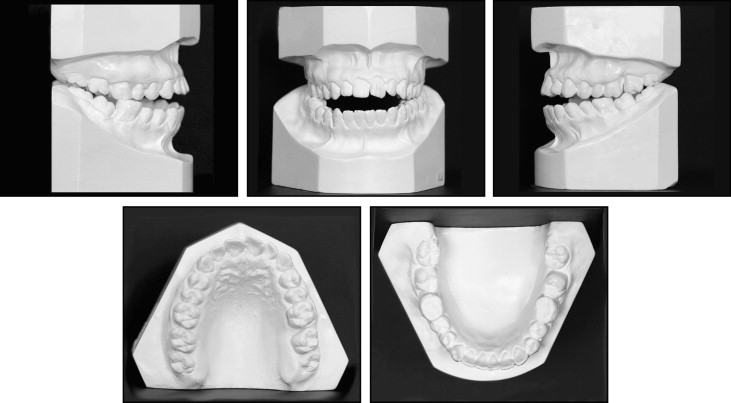
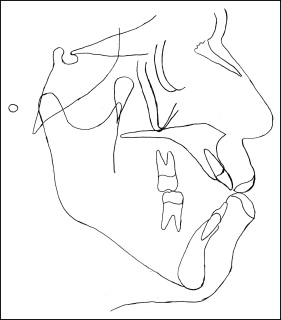
At the initial orthodontic visit, it was observed that the patient had a convex soft-tissue profile with a significantly increased lower third of the face ( Fig 1 ). The nasolabial angle was acute, and the lower lip was protrusive relative to Ricketts’ E-plane. At rest, his lips were apart, and a mentalis strain was observed. From the frontal view, his face was slightly asymmetric, with the right side a little longer than the left side, and the chin slightly deviated toward the left. The mandibular asymmetry could also be observed on the initial lateral cephalometric x-ray ( Fig 2 ). When smiling, the patient had uneven gingival margin levels. Intraoral and dental cast examinations showed a molar half-cusp Angle Class III relationship on both sides ( Fig 3 ). Overeruption (extrusion) of all maxillary and mandibular first molars was observed. An 8-mm anterior and a 3-mm bilateral posterior open bite were detected. The only teeth in contact were the extruded first molars and the third molars on both sides. A mesial inclination of the mandibular second molars developed, possibly because of the extrusion of the first molars. A significant tongue thrust and an anterior tongue rest posture were noticed at rest and also while swallowing. The maxillary arch was slightly narrow relative to the mandibular arch, possibly caused by the low and anterior tongue rest posture. Moderate maxillary anterior crowding and a small tooth-size discrepancy of the maxillary lateral incisors were observed. The temporomandibular joints had bilateral asymptomatic clicking, without deviation on opening, and no history of jaw locking in the closed position.
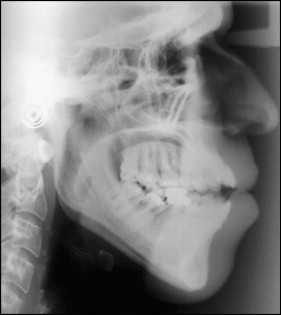
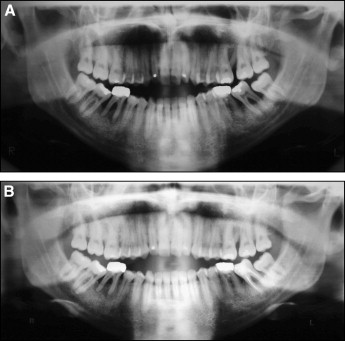
A panoramic film taken a year earlier by the periodontist and the initial orthodontic panoramic film showed the extension of the periodontal involvement of the molars ( Fig 4 ). A periapical lesion of the mandibular right first molar, periodontal pockets corresponding to the maxillary and mandibular left first and second molars and the mandibular right first molar, and a carious lesion on the mandibular left second molar were present. The severe bone loss surrounding the maxillary left first molar, the mandibular right and left first molars, and the second molars could be seen on the panoramic film taken by the periodontist ( Fig 4 , A ). One year later ( Fig 4 , B ), after periodontal treatment, the bone level had improved, and the mandibular left second molar had been endodontically treated. All third molars were present in the mouth. The pretreatment cephalometric tracing measurements showed an ANB angle of 1.4° ( Fig 5 , Table ). A vertical growth pattern was present, and the anterior portion of the mandible also had a vertical tendency. The mandibular plane angle was steep (SN-MP, 40.8°) possibly because of the extrusion of the first molars, adding to the vertical component. The maxillary incisors were extremely proclined (U1-FH, 119.6°), but the mandibular incisors were within normal limits (L1-MP, 89°).
| Initial | Final | Difference | Norm | |
|---|---|---|---|---|
| Maxilla to cranial base | ||||
| SNA (°) | 83.9 | 84.2 | 0.3 | 82 |
| Mandible to cranial base | ||||
| SNB (°) | 81.2 | 81.3 | 0.1 | 80 |
| SN-MP (°) | 40.8 | 39 | 1.8 | 32.9 |
| FMA (MP-FH) (°) | 37.8 | 33.7 | 4.1 | 22.9 |
| Maxillomandibular | ||||
| ANB (°) | 2.6 | 2.8 | 0.2 | 1.6 |
| Y-axis (°) | 70.1 | 68.9 | 1.2 | 60 |
| Maxillary dentition | ||||
| U1-NA (mm) | 9.2 | 2.1 | 7.1 | 4.3 |
| U1-SN (°) | 119.3 | 101.4 | 17.9 | 103.1 |
| Mandibular dentition | ||||
| L1-NB (mm) | 11 | 3.5 | 7.5 | 4 |
| L1-MP (°) | 88.9 | 81.6 | 7.3 | 95 |
| Soft tissue | ||||
| Lower lip to E-plane (mm) | 5.2 | 0.6 | 4.6 | −2 |
| Upper lip to E-plane (mm) | −1 | −2.3 | 1.3 | −8 |
Treatment objectives
The primary treatment objectives were to obtain a harmonious facial profile, close the open bite, and establish a normal occlusion with all teeth having a normal periodontium. To achieve these objectives, the periodontally compromised first molars were to be extracted and the remaining spaces closed. Because of the extractions of the extruded first molars and the mesial orthodontic movement of the posterior teeth, the open bite was expected to close significantly from the scissor, or drawbridge, effect. The anterior tongue rest posture was to be modified using a mandibular lingual arch with soldered tongue spurs. Since the posterior portion of the tongue was also abnormally postured in the extraction spaces, tongue spurs would be added in the area of those spaces. The mandibular left second molar would be monitored with the intent to salvage it. If in the future this tooth needed to be extracted because of periodontal considerations, space for an implant would be maintained. Although significant mesial orthodontic movement of second and third molars was required, it was expected that the spaces would remain closed after orthodontic treatment.
Treatment objectives
The primary treatment objectives were to obtain a harmonious facial profile, close the open bite, and establish a normal occlusion with all teeth having a normal periodontium. To achieve these objectives, the periodontally compromised first molars were to be extracted and the remaining spaces closed. Because of the extractions of the extruded first molars and the mesial orthodontic movement of the posterior teeth, the open bite was expected to close significantly from the scissor, or drawbridge, effect. The anterior tongue rest posture was to be modified using a mandibular lingual arch with soldered tongue spurs. Since the posterior portion of the tongue was also abnormally postured in the extraction spaces, tongue spurs would be added in the area of those spaces. The mandibular left second molar would be monitored with the intent to salvage it. If in the future this tooth needed to be extracted because of periodontal considerations, space for an implant would be maintained. Although significant mesial orthodontic movement of second and third molars was required, it was expected that the spaces would remain closed after orthodontic treatment.
Treatment alternatives
A combined maxillary and mandibular surgical approach, associated with extraction of the first molars, could have facilitated bite closure. However, the patient had previously consulted 4 orthodontists; all had recommended an orthognathic surgical procedure to correct his problem, but he vehemently rejected surgery. Tongue spurs combined with extraction of the maxillary and mandibular third molars, and maintenance of the first molar spaces for future implants, could have shortened the treatment time significantly. However, the treatment cost would have been significantly increased because of the required restorative work. A tongue crib could have been used instead of tongue spurs to impede the tongue from posturing forward and thus helping to close the bite. However, the anterior tongue posture might have relapsed after crib removal because a new engram would probably not have been established.
Treatment progress
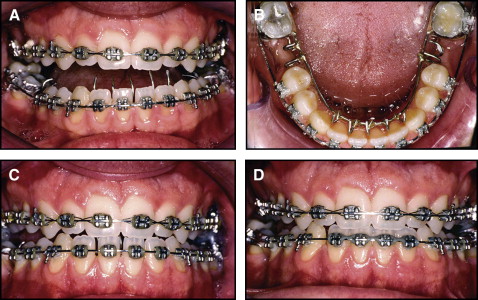
Before orthodontic treatment, the carious lesion was eliminated and the molar was restored with a filling; periodontal deep root scaling was performed, and instructions on oral hygiene were given. All maxillary and mandibular first molars were extracted. Bonded maxillary and mandibular 0.018 × 0.028-in slot Roth prescription Discovery brackets (Dentaurum USA, Newtown, Pa) were used to initiate leveling and alignment. After the initial treatment stages, a mandibular lingual arch was soldered onto the second molar bands, which were then cemented. The lingual arch had anterior and posterior tongue spurs soldered onto it ( Fig 6 , A and B ). The anterior open bite closed in a 4-month period without anterior vertical elastics. However, Class III elastics (bilateral triangular 5/16 in, 4 oz) were used and might have contributed to the bite closure. Closing the maxillary first molar spaces and modifying the anterior tongue rest posture habit also contributed to the treatment success ( Fig 6 , C and D ). The removal of the mandibular lingual arch and subsequent first molar space closure with elastomeric chains helped to close the anterior open bite because of the scissor effect. Class II elastics (3/16 in, 4 oz) were also used to help close the mandibular spaces by mesialization of the mandibular second molars. After the first molar extractions, the patient developed a habit of posturing the tongue into those newly created spaces. Tongue spurs were added to that area to prevent this new habit. Unlike the anterior tongue spurs, the posterior tongue spurs bothered the patient for more than 2 weeks.