This article reports the case of a 12-year-old patient with tooth extrusion, pain, gingival bleeding, and localized periodontitis near the maxillary second premolar. Despite probing and radiographic examination, it was not possible to establish the etiology. Tooth extraction was indicated because of the severe tooth mobility and extrusion. Curettage of the tooth socket revealed a rubber separator. Preventive approaches are suggested to avoid iatrogenesis and legal problems.
The consequences of invasion of the gingival sulcus and periodontal ligament by orthodontic elastics have been reported. Many of these reports describe problems that occurred during closure of diastemas with elastics applied directly to the incisor crowns. The elastics can slide on the tooth crown because of the lack of stabilization and then penetrate the gingival sulcus, causing tooth mobility, bone loss, and gingival retraction. These problems are treated by basic periodontal therapy, flap surgery, and splinting of the affected teeth, but in some cases the tooth is lost because of the severity of the lesion. Other reports have described cases of periodontitis secondary to the invasion of elastics in molars. The prognosis in molars is better because of the greater number of roots and also because the roots are divergent, whereas anterior teeth have more conical roots, facilitating the penetration of elastics and periodontal destruction.
An experimental study investigated the histopathology of periodontal lesions induced by elastics placed in the gingival sulcus of monkeys. After 2 to 4 weeks, the inflammation extended to the attached gingiva, and there were bleeding on probing, pockets of 5 to 8 mm, tooth extrusion, and horizontal and vertical bone loss. After the elastics were removed, the signs of inflammation and tooth mobility improved, yet there was no return to the conditions observed before placement of the elastics, and the pocket and bone destruction persisted.
Even though this event is well reported in the literature, invasion of the periodontal space by rubber separators is not a common finding. Because the placement of rubber separators is routinely performed in orthodontic practices, its iatrogenic potential should not be overlooked. We report a case of tooth loss caused by invasion of the periodontal ligament by a rubber separator and discuss some of the options available to prevent this accident.
Case report
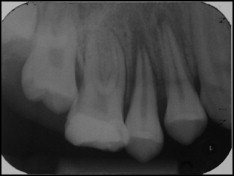
A 12-year-old boy who was receiving orthodontic treatment in a private practice dental office came to the emergency service of the Pediatric Dentistry Clinic at Araraquara Dental School in Brazil with a complaint of pain and difficulty in chewing. The clinical examination showed significant extrusion of the maxillary right second premolar, preventing occlusion of the teeth, and localized gingival inflammation, as well as cement on the smooth surfaces of the maxillary right first molar ( Figs 1 and 2 ). The radiographic periapical examination showed enlargement of the periodontal space, and the root apex had moved from the bottom of the tooth socket ( Fig 3 ).


The patient reported that a rubber separator had been placed between the maxillary right second premolar and first molar, but it could not be found after 2 days; painful symptoms developed at the same time. When the orthodontist was unable to find the rubber separator, he placed another in the same site. After a week, the second rubber separator was removed, and bands were cemented on the maxillary first permanent molars. The patient reported that the pain was still intense after banding, both at the site and in the temporomandibular joint region. There was extensive inflammation on the subsequesnt days, and the band was removed. After 9 days, the symptoms persisted, and the patient went to the emergency service at Araraquara Dental School.
After infiltrative anesthesia, a buccal gingival flap was raised, and periodontal probing was performed ( Fig 4 ). Tooth repositioning was then attempted. When these procedures were unsuccessful, it was decided to extract the tooth; the rubber separator was found during curettage of the tooth socket ( Fig 5 ).


Discussion
Tooth separation for banding of teeth is a routine procedure in orthodontic clinics. Patients also often return for banding without the rubber separators between their teeth. This commonly occurs because the interproximal space is increased, and the rubber separator is consequently lost during eating or brushing, and the loss is unnoticed by the patient. However, this case calls attention to the possible invasion of the periodontal space by rubber separators. When the rubber separator is missing at the banding appointment, it is advisable to determine whether the separator was actually removed. The patient might report that the rubber separator was missing, but in some cases the patient might not have noticed it. If there are complaints of pain, localized acute periodontitis, and gingival bleeding associated with tooth mobility or extrusion, the professional should consider the possibility of subgingival displacement of the rubber separator.
Rubber separators are commonly left in the mouth for 1 week ; they can cause enough discomfort to require the prescription of analgesic drugs. However, enough space for banding is achieved when rubber separators are placed for only 12 hours before the session, and the patient should be instructed to come to the office 3 to 4 hours before the appointment for separator replacement if the separator was lost. A shorter time of rubber separators in the mouth could be a better measure to prevent accidents, as reported here. Because the peak pain occurs 24 hours after separator placement, the discomfort to the patient and the risk of accidents like this might be minimized if rubber separators are used for only 12 hours before banding associated with prescription of analgesic drugs. Studies have demonstrated that, after 5 to 7 days, pain returns to the threshold levels observed before separator placement. However, banding in this period would imply exposing the patient to pain for nearly a week, and it also increases the risk of accidents as reported here.
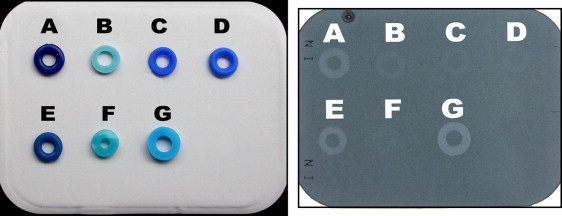
The periapical radiographic examination did not show a foreign body in the periodontal ligament region. Observation of the rubber band was not possible because of its lack of radiopacity. In this report, the cause of periodontitis was only elucidated after tooth extraction and curettage of the tooth socket, notwithstanding the placement of 2 rubber separators at the same site. Because of several reports of problems related to periodontal invasion by rubber separators, 1 suggestion would be to use radiopacifiers in the manufacture of rubber separators to allow for radiographic diagnosis. Even though this characteristic is desirable, not all commercially available rubber separators have this property. Figure 6 shows the radiographic images of some brands with varying degrees of radiopacity. The use of more radiopaque rubber separators would be advisable.