Introduction
This retrospective study was designed to investigate the position changes and movement patterns of incisors and molars after orthodontic treatment with extractions of 4 second premolars in patients with mild crowding, slight dental protrusion, and Angle Class I relationship.
Methods
Pretreatment and posttreatment cephalograms of 26 subjects were chosen from patients treated by an experienced orthodontist. The movements of the incisors and the molars as well as tooth tipping were measured.
Results
Relative to the posttreatment occlusal plane, the mean incisor movements were 3.3 and 2.9 mm lingually in the maxilla and the mandible, respectively. The first molars were moved mesially an average of 3.2 and 3.4 mm in the maxilla and the mandible, respectively. The incisor inclination was under proper control. The extraction space was almost equally taken up by the anterior and posterior segments.
Conclusions
These data can be used to estimate the expected position changes and movement patterns of the incisors and molars in patients with mild crowding and slight bialveolar dental protrusion after orthodontic treatment with 4 second premolar extractions.
The first premolar has been the most common tooth removed in orthodontic clinics, as suggested by previous articles. But, in some patients with mild crowding, acceptable incisor positions and facial profiles, the second premolar would be an alternative to the first premolar to be extracted. Nance was one of the first to propose this; underlying his and some other advocates’ recommendations was the concept that second premolar removal would result in less incisor retraction and consequently less lip retraction compared with first premolar removal. It is widely accepted that the anchorage potential is highly related to the area of root surface involved. Proffit figured out that less incisor retraction effect would be anticipated while extracting the further posteriorly located tooth. And the space of second premolar extraction was mainly occupied by mesial movement of the molars, but some retraction of the incisor could occur. This incisor retraction effect has been confirmed by other researchers.
Despite the agreement that improvement in orthodontic techniques increases the potential to freely move teeth 3 dimensionally and to correlate these movements with expected facial growth changes, it is still believed that a particular premolar removal will have predictable incisor and molar position changes. Diagnosis and treatment planning are based on this prediction; accordingly, the plan is executed to ensure that the teeth will ultimately reside in the predetermined positions.
When reviewing studies that examined the effects of second premolar extraction treatment on tooth movement, we found that most reports were based on clinical observations; there is little scientific information to make an accurate prediction of extraction space distribution. Also, controversy surrounds the distances of incisor and molar movement. Some authors reported little, if any, incisor change, and the extraction site was almost taken up by molars. But others found that the incisors were retracted remarkably, even as much as 3 mm. Underlying this inconsistent phenomenon is the complexity of the subjects studied. There were considerable differences in the pretreatment characteristics in a study and between studies, including severity of crowding, arch discrepancy, vertical skeletal pattern, and other orofacial features, which resulted in the wide range of individual variations in tooth movement. One example was that subjects with blocked-out and impacted second premolars were included in the study of Schoppe. Since severity of crowding, pretreatment incisor position, FMA angle, and individual response can influence the distance of incisor movement, it would, therefore, seem to be impossible to predict the incisor movement in a patient according to the average data obtained from a group of subjects with various craniofacial features, as suggested by previous authors.
To observe tooth response, it is appropriate to study patients with normodivergent facial type, mild or no crowding, and Angle Class I relationship. In hyperdivergent or hypodivergent subjects, the skeletal pattern might affect horizontal tooth movement. In those with severe crowding, most extraction space would be used to reconcile arch length discrepancy, and then the space distribution pattern would be affected by the amount of residual space and the mechanotherapy used in releasing crowding. Class I malocclusions were selected to eliminate excessive molar movement involved in the treatment of Class II and Class III malocclusions.
Therefore, this study was undertaken to determine the anterior and posterior dental changes in a group of patients with mild crowding, slight dental protrusion, and Angle Class I relationship treated with 4 second premolar extractions and preadjusted appliances.
Material and methods
This study was retrospective and included 26 subjects: 15 boys and 11 girls, with an average age of 16 years 1 month at the commencement of treatment and an average treatment time of 2 years 1 month.
All subjects were selected from patients referred to the Department of Orthodontics, West China Stomatology Hospital, Sichuan University, who fulfilled the following criteria: (1) skeletal Class I and dental Class I malocclusion, (2) mild arch crowding (0-4 mm), (3) slight dental bimaxillary protrusion, and (4) normodivergent face type (24° <FH-MP <34°).
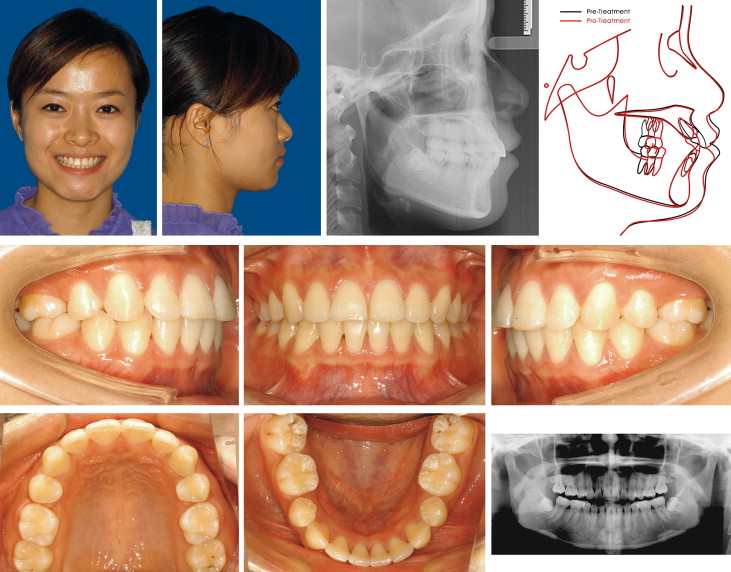
This clinical research was approved by the institutional ethics review board of Sichuan University. The pretreatment characteristics of the subjects are shown in Table I . All patients were diagnosed and treated by 1 operator (D.B.) with a 0.028-in slot preadjusted edgewise appliance (Roth) and sliding mechanics. The treatment protocol was as follows: 4 second premolars were extracted as part of a comprehensive orthodontic treatment plan. All teeth mesial to the second molar were bonded. A preadjusted edgewise appliance was used for all patients. After aligning the maxillary and mandibular dental arches with sequentially changed continuous nickel-titanium archwires, maxillary and mandibular 0.018 × 0.025-in stainless steel wires with a reverse curve of Spee were placed with a depth of about 3 to 4 mm. The crown labial torque in the maxillary posterior and mandibular wires was eliminated, but maintained in the maxillary anterior part. The crown labial torque was about 10° in the maxillary central incisor region. On these wires, intra-arch nickel-titanium coil springs were used to close the remaining spaces, and interarch Class II elastics were used when required to harmonize the molar relationship. After all spaces were completely closed, the second molars were included in the archwire, and the whole arches were aligned again. No posterior anchorage enhancement appliance (eg, temporary implant anchorage or transpalatal arch) was used. Normal incisor overbite and overjet and posterior neutral relationships were achieved at the end of treatment. One patient’s records are shown to illustrate the pretreatment orofacial features and treatment changes ( Figs 1 and 2 ).
| Variable | Before treatment | After treatment | Significance ( P value) |
||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age at start (y) | 16.1 | 4.3 | |||
| Crowding (mm) | 2.0 | 1.3 | |||
| SNA (°) | 84.1 | 4.2 | 83.6 | 4.3 | 0.1204 |
| SNB (°) | 80.6 | 4.5 | 80.3 | 4.8 | 0.4037 |
| ANB (°) | 3.5 | 1.9 | 3.3 | 1.5 | 0.315 |
| FMA (°) | 29.4 | 6.8 | 29.5 | 7.2 | 0.7141 |
| OP/SN (°) | 18.1 | 5.6 | 18.3 | 5.6 | 0.8383 |
| U1/PP (°) | 59.1 | 8.2 | 68.0 | 10.0 | 0.0002∗ |
| U6/PP (°) | 78.5 | 10.1 | 80.4 | 5.2 | 0.429 |
| U1/NA (°) | 25.3 | 5.9 | 18.5 | 6.6 | 0.0009∗ |
| U1-NA (mm) | 5.0 | 2.3 | 2.5 | 1.9 | 0.0003∗ |
| L1/MP (°) | 93.4 | 8.1 | 88.3 | 6.5 | 0.005∗ |
| L6/MP (°) | 84.3 | 5.2 | 80.3 | 6.0 | 0.003∗ |
| L1/NB (°) | 31.6 | 5.2 | 26.8 | 5.0 | 0.0051∗ |
| L1-NB (mm) | 7.4 | 1.6 | 5.3 | 1.7 | 0.0003∗ |
| U1/L1 (°) | 118.6 | 9.2 | 130.4 | 8.7 | 0.0003∗ |
| Upper lip to E-line (mm) | 2.7 | 1.4 | 1.5 | 2.0 | 0.031∗ |
| Lower lip to E-line (mm) | 4.1 | 2.1 | 2.1 | 2.3 | 0.015∗ |
| Z angle (°) | 79.4 | 3.7 | 76.6 | 3.7 | 0.032∗ |

Patients whose second premolars were extracted for other reasons, such as severe caries, periapical lesions, or blocked out or impacted teeth, and who had systemic diseases that could affect bone metabolism were excluded from this study.
Lateral cephalometric radiographs were taken of all patients before and after treatment. The cephalograms were obtained on the same radiographic unit (Orthopantomograph OP 100D, Instrumentarium, Tuusula, Finland) under standardized conditions.
The amounts of incisor and molar movement were assessed by superimposing the maxilla on ANS and the palatal plane (ANS-PNS), and the mandible by the structural method. Retraction of the maxillary and mandibular central incisors was measured on the posttreatment occlusal plane, from the projection point of the maxillary and mandibular central incisors’ edge and apex. The degrees of maxillary and mandibular incisor tipping were measured from the angle between the long axis of the incisor and the palatal plane and mandibular plane, respectively. Molar movement was measured from a perpendicular between the posttreatment occlusal plane and the most mesial point on the molar crown and the mesial apex. The degrees of maxillary and mandibular molar tipping were measured from the angle between the long axis of the mesial root and the palatal plane and mandibular plane, respectively ( Fig 3 ). All tracing and measuring work was done by the same operator (K.C.).
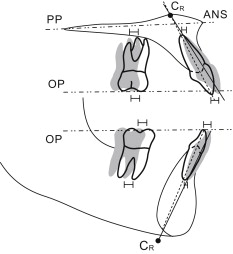
The center of rotation of the incisors can be determined by the method of Christiansen and Burstone as the intersection of 2 lines that coincides with the tooth axis before and after treatment ( Fig 3 ).
Statistical analysis
Statistical analysis, including calculations of the means and standard errors of the mean for each variable, was conducted with SPSS software (version13.0, SPSS, Chicago, Ill).
Ten randomly selected cephalograms were retraced and measured twice 4 weeks apart. Results of the paired Student t test showed no significant difference between the 2 sets of measurements at the 95% CI.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


