Introduction
Although natural head position has proven to be reliable in the sagittal plane, with an increasing interest in 3-dimensional craniofacial analysis, a determination of its reproducibility in the coronal and axial planes is essential. This study was designed to evaluate the reproducibility of natural head position over time in the sagittal, coronal, and axial planes of space with 3-dimensional imaging.
Methods
Three-dimensional photographs were taken of 28 adult volunteers (ages, 18-40 years) in natural head position at 5 times: baseline, 4 hours, 8 hours, 24 hours, and 1 week. Using the true vertical and horizontal laser lines projected in an iCAT cone-beam computed tomography machine (Imaging Sciences International, Hatfield, Pa) for orientation, we recorded references for natural head position on the patient’s face with semipermanent markers. By using a 3-dimensional camera system, photographs were taken at each time point to capture the orientation of the reference points. By superimposing each of the 5 photographs on stable anatomic surfaces, changes in the position of the markers were recorded and assessed for parallelism by using 3dMDvultus (3dMD, Atlanta, Ga) and software (Dolphin Imaging & Management Solutions, Chatsworth, Calif).
Results
No statistically significant differences were observed between the 5 time points in any of the 3 planes of space. However, a statistically significant difference was observed between the mean angular deviations of 3 reference planes, with a hierarchy of natural head position reproducibility established as coronal > axial > sagittal.
Conclusions
Within the parameters of this study, natural head position was found to be reproducible in the sagittal, coronal, and axial planes of space. The coronal plane had the least variation over time, followed by the axial and sagittal planes.
Natural head position (NHP) was first described by Broca in 1862 as a stable physiologic position “when a man is standing and his visual axis is horizontal.” In 1958, Moorrees and Kean defined it more specifically as “a standardized and reproducible orientation of the head in space when one is focusing on a distant point at eye level.” As potential applications of NHP in cephalometric analysis were demonstrated, the claims of standardization and reproducibility came under greater scrutiny; however, numerous studies supported the stability of each patient’s NHP in the sagittal plane. Bjerin and Moorrees and Kean found deviations ranging from 1.3° to 2°; Lundström et al found variations of 1.5° to 2° using cephalometric radiography combined with photography, and Cooke and Wei found a 1.9° deviation using a mirror for orientation. In the latter study, cephalograms repeated 15 years later demonstrated a 2.2° deviation from the baseline measurements. Although most research supports the reproducibility of NHP, deviations were reported by Vig et al in patients with total nasal obstruction and by Achilleos et al as a physiologic adaptation to orthognathic surgery. However, in the latter study, NHP was restored to its original position 1 year postsurgery.
Methods to record NHP have varied in the literature; however, a cephalometric radiograph with a plumb line chain was first used and proved to be easily incorporated into clinical practice. Other methods have involved more complicated instrumentations, such as registration jigs, eyeglasses with inclinometers attached to the frames, and 3-dimensional laser scanners to record NHP.
Stimulated by the recent increased interest in 3-dimensional cone-beam computed tomographic imaging for orthodontic evaluation, studies demonstrating and testing various methods to record NHP 3 dimensionally have appeared in the literature. Xia et al used stereolithographic skull models of patients to demonstrate the 3-dimensional reproducibility of NHP. Recently, Koerich de Paula et al tested the effectiveness of minisensors in capturing changes with 6 degrees of freedom using NHP and stereophotogrammetry. Although their study demonstrated that the reproducibility of NHP is enhanced with the use of sensors, they concluded that spatial head position acquisition still requires additional registration procedures.
Although the use of 3-dimensional cone-beam computed tomography (CBCT) offers certain diagnostic advantages over conventional 2-dimensional cephalometric analysis, there are difficulties in orienting the volume in existing 3-dimensional imaging software programs because of the absence of external references during the CBCT acquisition process. Additionally, to reduce the amount of motion artifacts during the image acquisition process, it is helpful to use a head strap to restrain the patient’s head to the headrest, especially in younger patients. Any head restraint device, however, would obviously affect the patient’s physiologic head position. As an alternative, Cevidanes et al presented a method of positioning the CBCT volume in the software with a simulated NHP, but it was not a true physiologically based head position.
Because of limitations in conventional 2-dimensional methodology and the need for additional radiographic images, few studies have evaluated NHP in 3 planes of space. However, with stereophotogrammetry, it is now possible to evaluate the reproducibility of the coronal, sagittal, and axial planes of space without cephalometric radiography. This study was designed to expand on the known reproducibility of NHP in the sagittal plane and to evaluate reproducibility in the coronal and axial planes over time by using a simplified technique that could be applied to the CBCT acquisition process.
Material and methods
Twenty-eight adult active-duty military personnel, aged 18-40 years, were selected to participate in this longitudinal study conducted at the 3-dimensional imaging department at the Tri-Service Orthodontic Residency Program, Joint Base San Antonio, Lackland Air Force Base in San Antonio, Tex. The protocol was approved by the biomedical institutional review board, and informed consent was obtained from all subjects.
A studio was created to facilitate standardized light conditions and support all necessary equipment. As illustrated in Figure 1 , the subjects were asked to sit in an iCAT CBCT machine (Imaging Sciences International, Hatfield, Pa), but no radiographic scans were taken of the subjects. The iCAT device was only used as a reference to place orientation ink points on the faces by using the machine’s laser light beams projected to register true horizontal and vertical lines. Adjustments to seating heights were made to assist the subjects in achieving proper placement of the laser lines on their faces.

The subjects were asked to tilt their heads forward and backward with decreasing amplitude until they came to a comfortable position, and a natural head balance was reached. Once they were comfortable, they were asked to look directly into their own eyes in a mirror, which was mounted on a door directly in front of them at a distance of 7 feet, and finalize their head position.
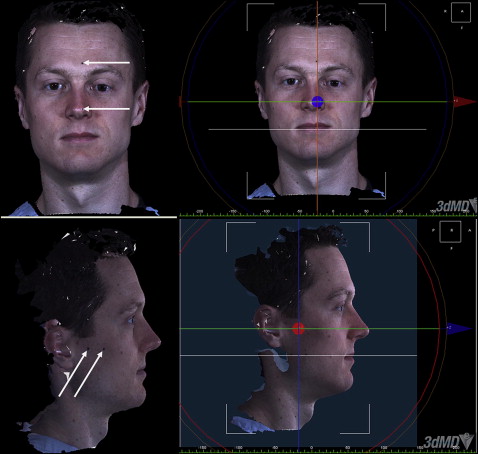
By using semipermanent Sharpie markers (Newell Rubbermaid Office Products, Oak Brook, Ill), 4 ink dots were placed along the laser light beams: 2 dots were placed in the vertical plane along the forehead and on the midface including the tip of the nose, and 2 dots were placed in the horizontal plane on the preauricular and infrazygomatic areas. The subjects were then escorted to the photographic area for facial imaging with the stereophotographic imaging system (3dMD, Atlanta, Ga) as illustrated in Figure 2 . At each time point, the process was repeated, placing dots to register NHP, followed by a 3-dimensional photograph. Photographs were taken at 5 times: initial baseline, and 4 hours, 8 hours, 24 hours, and 1 week later.

Three-dimensional surface images were obtained by using the Face multicamera system (3dMD), which was calibrated before each imaging session. The stereophotography unit uses 4 cameras: 2 positioned on either side of the subject. It covers a 180° face capture (ear to ear), has a capture speed of 1.5 ms at the highest resolution, and is reported by the manufacturer to have a clinical accuracy of 1.5% of total observed variance.
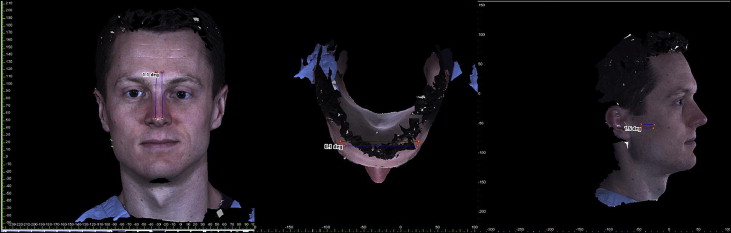
All photographic images were exported as .tbs files and imported into the 3dMDvultus imaging software (3dMD) in which digital models were reconstructed from the data, and the ink dots were digitized. As illustrated in Figure 3 , the initial image was oriented to align the digitized ink dots with the axial and sagittal planes in the software and then digitally locked to the image with the software tools. The coronal plane was established as the resultant perpendicular to both the axial and sagittal planes. Two points were then digitized on the computer-generated coronal plane and locked in place with the software tool. A line segment was constructed connecting the 2 digitized points in each plane for comparison with future time points.
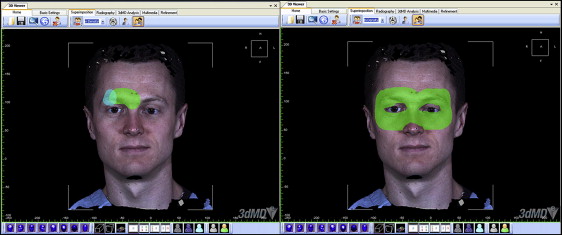
Subsequent facial images (4 hours to 1 week later) of each subject were superimposed over the baseline image to determine changes in the 3 dimensions of space for each time interval. As illustrated in Figure 4 , with the 3dMDvultus imaging software, a systematic process was used by manually aligning the facial photographs on a subject’s forehead (brow area) and under the eyes, as described by Incrapera et al. The images were superimposed by using the broadest area of the anterior position of the forehead, including soft-tissue glabella, soft-tissue nasion, and the bridge of the nose to incorporate a regional fit environment.
Screen captures were completed for all superimpositions in the sagittal, axial, and coronal planes to capture the relationship of the 2 lines observed on the 2 superimposed images. These screen captures were exported into software (Dolphin Imaging & Management Solutions, Chatsworth, Calif) as .jpeg files. Angular differences were measured between the 2 lines as depicted in Figure 5 . The Dolphin Imaging software was used because of its ability to measure closely parallel lines with 4 digitized points (2 points digitized on each line segment from the separate time point images that were superimposed).