Introduction
The aim of this study was to compare the accuracy of dental measurements taken with calipers on plaster dental casts and those from computed tomography scans of the dentition with a dental measurement program.
Methods
The sample consisted of plaster dental models of 34 orthodontic subjects. Dental arch measurements, including mesiodistal widths of teeth, arch widths, arch lengths, arch perimeters, and palatal depths were made with the calipers. The patients were also scanned with computed tomography, and measurements were made digitally with a 3-dimensional-based dental measurements program (3DD, Biodent, Cairo, Egypt).
Results
The results showed strong agreement in most measurements between the conventional method and the 3DD in the 3 planes of space. The mesiodistal measurements of the maxillary right and left second premolars, left central incisor, and right first molar, and the mandibular left and right central incisors, right canine, and left first premolar had fair agreement.
Conclusions
Excellent agreement between the measurements with the conventional and 3DD methods in the 3 planes of space was found; 3DD can be an alternative to conventional stone dental models.
Successful orthodontic treatment is based on extensive diagnosis and treatment planning. Dental models, photographs, radiographs, and clinical examinations provide essential information for diagnosis. Study casts are a standard component of orthodontic records and are fundamental to diagnosis, case presentation, treatment planning, evaluation of treatment progress, and record keeping. Tooth size, crowding or spacing, overjet, overbite, and Bolton analysis are typically measured manually on models.
Digital photographs and radiographs are now routinely incorporated into electronic files, but digital dental models are not as widely used. Electronic storage of patient information, including study models, eliminates problems of physical storage, retrieval, maintenance, and office management. Documentation of treatment progress and communication between professional colleagues can be enhanced by digital records.
Attempts have been made to transform dental plaster models into 3-dimensional (3D) virtual models. OrthoCAD (Cadent, Carlstadt, NJ) is a commercially available system that transforms casts or impressions into 3D digital models. Tomassetti et al evaluated various measuring methods, including OrthoCAD, to analyze the Bolton tooth size discrepancy. OrthoCAD values were found to be less correlated to the baseline values established by the average of 3 repeated measurements with a Boley gauge.
The SureSmile (OraMatrix, Dallas, Tex) process begins with a direct clinical 3D scan of the patient’s dentition with the OraScanner (OraMatrix), a light-based imaging device that projects a precise patterned grid onto the teeth. The orthodontist can then diagnose and plan treatment on the computer screen, using software tools to measure tooth and arch dimensions, and create symmetric and asymmetric archforms.
Several studies were conducted to compare 3D virtual models with plaster models. Stevens et al compared the analysis of the gold-standard plaster model with the digital counterpart of the e-model (GeoDigm) for tooth sizes and occlusal relationships, specifically the Bolton analysis and the peer assessment rating index. Strong agreement between the measurements indicated that the digital models are a good replacement for conventional plaster models.
Whetten et al investigated the difference between plaster models and the virtual 3D model (e-model) in treatment planning for Class II patients. They concluded that digital orthodontic study models (e-models) were a valid alternative to traditional plaster models in treatment planning for these patients.
The aims of this study were to test the accuracy of a 3D-based dental (3DD) measurement program (Biodent, Systems and Biomedical Engineering Department, Faculty of Engineering, Cairo University, Cairo, Egypt) that uses computed tomography (CT) scans and to compare it with manual measurements made on plaster models.
Material and methods
Our sample consisted of 34 adults, equally divided between men and women. Their ages ranged from 20 to 25 years. Approval for this study was obtained from the hospital Board of Research Ethics. All subjects had erupted permanent dentitions from the first molar of one side to the first molar of the other side, with no orthodontic appliances. Measurements were recorded on both the conventional model and the 3D virtual model from the CT scan with a blind protocol.
For the conventional plaster models, the maxillary and mandibular casts of the 34 subjects were measured with Vernier calipers (OISt Orthodontics, Aston, Pa) calibrated to the nearest 0.1 mm.
For the 3D virtual models, each subject’s head was scanned with a DCT device (Light Speed Pro, General Electric medical CT scan machine, Wakesha, Wis) at an axial section of 1.25 mm. Effective milli-amperage was based on the preliminary scanogram, 80 mAs, spiral scanning of 120 Kv, high resolution mode. The reconstruction interval was 0.6 mm with table feed of 17.5 mm per rotation. The total rotation time was 15 to 20 seconds. During the CT scanning, the subject was given a prefabricated splint (1 mm) to keep the maxillary and mandibular teeth separated; this was done to reproduce the occlusal anatomy and prevent blurring of the dental images. The inclination of the gantry was set parallel to the occlusal plane of the maxilla. All data were saved with a DICOM extension.
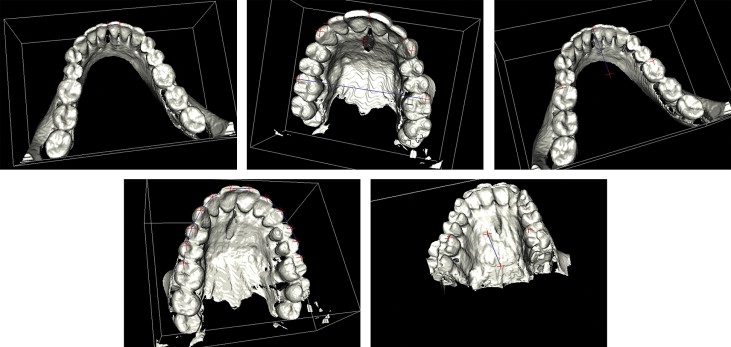
For the 3D reconstruction, custom-made 3D computer software (Biodent) was used to reconstruct the 3D volume from the axial CT scans and separate the maxillary and mandibular dentitions. This software is based on the concept of window center and window width (brightness and contrast) produced by CT scanners.
Measurements of the 3D volume were made with the measuring analysis tool of the 3DD program. For accuracy and ease of measurements, the images were enlarged on the screen by using a built-in magnifying tool.
From the occlusal view, the following dental arch measurements were taken for both the conventional casts and the 3D virtual models by the same observer (H.M.Z.) ( Fig 1 ).
- 1.
Mesiodistal tooth width from the first permanent molar of 1 side to the first permanent molar of the other side.
- 2.
Arch width, maxillary interlateral incisor width, mandibular interlateral incisor width, maxillary intercanine width, mandibular intercanine width, maxillary interfirst molar width, and mandibular interfirst molar width.
- 3.
Maxillary anterior arch length, mandibular anterior arch length, maxillary posterior arch length, and mandibular posterior arch length.
- 4.
Maxillary and mandibular arch perimeters.
- 5.
Maxillary palatal depth (from the distal view).
Replication of the measurements (for reliability testing) was done by the same observer (H.M.Z.). These intraobserver measurements were made a week after the first set of measurements for both the conventional and the 3D model.
Statistical analysis
The data were collected, tabulated, and analyzed. A reproducibility index, called the concordance correlation coefficient (CCC), introduced by Lin, was used. It evaluates the agreement between 2 readings (from the same sample) by measuring the variation for the 45° line through the origin (the concordance line). The CCC measurements are accurate and precise.
The CCC and the Pearson correlation coefficient (PCC) were used to evaluate the equivalence and association, respectively, between the conventional and digital measurements. Reproducibility for intraexaminer measurements was assessed with the CCC and PCC statistical test.
Results
The results and comparisons between the conventional and digital models are shown in Tables I through V . The results were compared for conformity and equivalency by using the CCC and PCC tests, respectively.
| Conventional | Digital | |||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | CCC | PCC | |
| Maxillary arch width (mm) | ||||||
| Interlateral incisor | 28.86 | 2.07 | 28.48 | 2.03 | 0.968 ∗ | 0.985 ∗ |
| Intercanine | 35.18 | 2.34 | 34.86 | 2.35 | 0.978 ∗ | 0.987 ∗ |
| Interfirst molar | 52.32 | 3.35 | 52.04 | 3.39 | 0.992 ∗ | 0.995 ∗ |
| Mandibular arch width | ||||||
| Interlateral incisor | 21.57 | 1.52 | 21.23 | 1.60 | 0.948 ∗ | 0.973 ∗ |
| Intercanine | 25.80 | 1.67 | 25.84 | 1.69 | 0.980 ∗ | 0.980 ∗ |
| Interfirst molar | 44.17 | 2.96 | 44.11 | 2.87 | 0.987 ∗ | 0.988 ∗ |
| Conventional | Digital | |||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | CCC | PCC | |
| Maxillary left mesiodistal tooth width (mm) | ||||||
| Central incisor | 8.71 | 0.583 | 8.54 | 0.560 | 0.79 ∗ | 0.828 ∗ |
| Lateral incisor | 6.71 | 0.591 | 6.69 | 0.610 | 0.811 ∗ | 0.812 ∗ |
| Canine | 7.47 | 0.539 | 7.45 | 0.555 | 0.821 ∗ | 0.822 ∗ |
| First premolar | 6.44 | 0.435 | 6.46 | 0.411 | 0.803 ∗ | 0.806 ∗ |
| Second premolar | 6.35 | 0.363 | 6.32 | 0.407 | 0.704 | 0.712 † |
| First molar | 10.15 | 0.594 | 10.18 | 0.447 | 0.845 ∗ | 0.882 ∗ |
| Maxillary right mesiodistal tooth width (mm) | ||||||
| Central incisor | 8.73 | 0.568 | 8.60 | 0.593 | 0.855 ∗ | 0.878 ∗ |
| Lateral incisor | 6.73 | 0.691 | 6.67 | 0.683 | 0.894 ∗ | 0.898 ∗ |
| Canine | 7.67 | 0.500 | 7.52 | 0.483 | 0.809 ∗ | 0.846 ∗ |
| First premolar | 6.51 | 0.477 | 6.53 | 0.401 | 0.761 ∗ | 0.773 ∗ |
| Second premolar | 6.25 | 0.393 | 6.35 | 0.413 | 0.674 † | 0.699 † |
| First permanent molar | 10.00 | 0.556 | 10.08 | 0.446 | 0.718 † | 0.746 † |
| Mandibular left mesiodistal tooth width (mm) | ||||||
| Central incisor | 5.42 | 0.401 | 5.28 | 0.373 | 0.659 † | 0.704 † |
| Lateral incisor | 5.67 | 0.510 | 5.56 | 0.458 | 0.826 ∗ | 0.854 ∗ |
| Canine | 6.54 | 0.476 | 6.57 | 0.495 | 0.784 ∗ | 0.786 ∗ |
| First premolar | 6.55 | 0.476 | 6.53 | 0.411 | 0.716 † | 0.725 † |
| Second premolar | 6.75 | 0.512 | 6.68 | 0.532 | 0.827 ∗ | 0.836 ∗ |
| First permanent molar | 10.30 | 0.551 | 10.33 | 0.546 | 0.837 ∗ | 0.838 ∗ |
| Mandibular right mesiodistal tooth width (mm) | ||||||
| Central incisor | 5.43 | 0.413 | 5.28 | 0.369 | 0.571 † | 0.617 † |
| Lateral incisor | 5.82 | 0.427 | 5.70 | 0.427 | 0.793 ∗ | 0.827 ∗ |
| Canine | 6.62 | 0.421 | 6.60 | 0.427 | 0.723 † | 0.723 † |
| First premolar | 6.59 | 0.540 | 6.54 | 0.614 | 0.884 ∗ | 0.894 ∗ |
| Second premolar | 6.74 | 0.449 | 6.70 | 0.464 | 0.881 ∗ | 0.885 ∗ |
| First permanent molar | 10.42 | 0.588 | 10.46 | 0.549 | 0.846 ∗ | 0.85 ∗ |
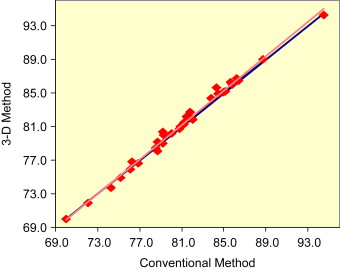
Excellent agreement was obtained between both measuring modalities for arch width. For maxillary arch width, the CCC ranged from 0.968 to 0.992, and the PCC was 0.985 to 0.995. Mandibular arch widths were 0.948 to 0.987 for the CCC and 0.973 to 0.988 for the PCC ( Table I ). For arch length, there was excellent agreement between the measurements with the 2 measuring modalities, with CCC values of 0.971 and 0.979 for maxillary anterior and posterior arch lengths, respectively. The PCC findings for the same parameter were 0.973 and 0.981, respectively. Comparable findings were observed with the CCC and PCC tests: 0.979 and 0.946 for mandibular anterior and posterior arch lengths, respectively ( Table II ). For the maxillary arch perimeter, the CCC and PCC values were 0.995 and 0.996, respectively ( Fig 2 ), and the value was 0.979 for the mandibular arch perimeter with both statistical tests ( Table III ).
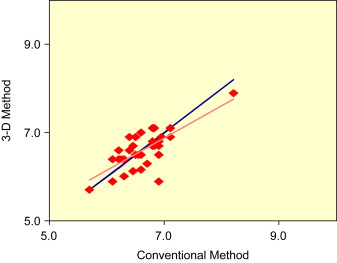
Measurements of the mesiodistal widths of most maxillary and mandibular teeth showed strong agreement between the conventional and 3DD modalities ( Table IV ). The values between the 2 modalities were 0.761 to 0.894 for the CCC test and 0.773 to 0.898 for the PCC test. The mesiodistal measurements of the following teeth showed fair agreement between the 2 measuring modalities: maxillary left second premolar (CCC, 0.704; PCC, 0.712), maxillary right second premolar (CCC, 0.674; PCC, 0.699), maxillary right first molar (CCC, 0.718; PCC, 0.746), mandibular left central incisor (CCC, 0.659; PCC, 0.704), mandibular right central incisor (CCC, 0.571; PCC, 0.617), mandibular right canine (CCC, 0.723; PCC, 0.723) ( Fig 3 ), and mandibular left first premolar (CCC, 0.716; PCC, 0.725). Results of the palatal depth measurements in Table V showed excellent agreement among the 2 computation modalities (CCC, 0.916; PCC, 0.933).