Schematic representation of the discussed irrigation techniques. Sketches of the various manual (a, b) and automated (c–e) irrigation techniques. For positive pressure irrigation, (a) both the open-ended (left) and closed-ended (right) needles are shown; negative pressure irrigation is shown in (b). Sonic (c) and ultrasonic activation (d) involves oscillating instruments (black-bended shapes) with one or more nodes and antinodes. For laser-activation irrigation, (e) the optical fiber is drawn. The typical flow velocities and patterns for all irrigation techniques are indicated as well
3.3 Operational Characteristics of the Irrigation Systems
3.3.1 Syringe Irrigation
As mentioned earlier, syringe irrigation is the most commonly used root canal irrigation procedure either as the sole irrigation technique or intermittent with other activation techniques [17]. During syringe irrigation, the irrigant is typically delivered by a needle connected to a syringe, with the needle tip preferably positioned as close to working length as possible [18]. There are various needle types available on the market, which can be categorized as open-ended (sharp or blunt end) or closed-ended (one or more side outlets) designs [12]. Various needle sizes are available, but most commonly used are the 27 and 30 gauge needles (respectively 0.4 and 0.3 mm outer diameter). Needles are made from stainless steel, NiTi, or flexible material like polyimide. The flow through the needle is generated by applying a pressure on the attached syringe [19]. Syringes are available at sizes ranging from 1 mL to 50 mL, with the smaller ones being more popular and easier to achieve high flow rates.
3.3.2 Negative Pressure Irrigation
Negative pressure irrigation systems make use of a microcannula that is placed in the middle part of the root canal or close to the working length [15]. Irrigant is aspirated through the cannula, while fresh irrigant is provided in the pulp chamber using a larger needle. Thus, the flow is directed from the pulp chamber to the aspirating cannula. The negative pressure systems involve less risk on irrigant extrusion through the apical foramen than positive pressure techniques due to the absence of a flow directed towards the foramen [20–22]. This technique is therefore considered safer than positive pressure syringe irrigation.
3.3.3 Laser Activation
One of the more recent techniques available for automated agitation/activation of irrigant in the root canal is laser-activated irrigation (LAI). This application uses laser energy to agitate and activate the irrigant. The lasers typically used for LAI are the erbium laser family such as ErCrYSGG and Er:YAG. These lasers have wavelengths in the medium-infrared region (2780–2940 nm) which is highly absorbed in water and NaOCl [23]. These laser devices cycle and pulse at frequencies anywhere 1–100 Hz with energy’s ranging from 5 to 1000 mJ per pulse. The laser light is delivered through an optical fiber or an articulated arm to a handpiece with a terminal flat or conical tip, suitable for insertion into the root canal close to the root apex. To be effective in the whole root canal, different LAI protocols are used to apply the laser tip in the different segments of the root canal. In a variation on this technique, the fiber tip is placed just above the root canal entrance, in the pulp chamber which is filled with irrigant [24, 25]. This leads to agitation/activation and streaming of the irrigant throughout the entire root canal system. This specific LAI technique, referred to as photon-induced photoacoustic streaming (PIPS), uses specially developed tapered and stripped laser fiber tips in combination with low energy (20 mJ) and short pulse duration (50 microseconds). These fibers allow lateral emission of the laser light at from the tip [25].
Pulse frequency and power do not appear to heat the root canal wall more the 5 C during laser activation [26]. Using the low pulse duration and energy as is recommended for PIPS protocol, the radicular apical third only increased 1.2 or 1.5 °C after 20–40 s of activation respectively [27]. This laser-activated irrigation is an indirect technique that utilizes photoacoustics for activation and agitation and not direct ablation of the biomaterial as seen in other applications [28].
3.3.4 Sonic Activation
Sonic activation employs instruments that are driven into vibration at one end (at the handpiece). The other (free) end of the instrument is inserted to near the working length of the root canal. The oscillations of the instruments agitate the irrigant inside the root canal in order to enhance mixing and cleaning of the irrigant by fluid flow.
Sonic devices operate at audible frequencies (below 20 kHz, typically 100 Hz for the current devices) [29]. The sonically driven instruments exhibit a simple bending pattern, consisting of a large amplitude at the tip (antinode) and a small amplitude at the driven end (node) [30]. The amplitude at the antinode may be as large as 1 mm, which is larger than the diameter of a root canal. Therefore, frequent wall contact is likely to occur, which reduces the effectiveness of the technique [29].
3.3.5 Ultrasonic Activation
Like sonic activation, the instruments used during ultrasonic activation have an enforced vibration at one end (at the handpiece) and are allowed to vibrate freely at the other end. The instruments are typically either cutting or non-cutting files. Recently, hollow instruments have been introduced, which allow for simultaneous ultrasonic oscillation and positive pressure irrigation [15].
Ultrasonic devices operate at higher frequencies (typically 20–200 kHz) and have amplitudes less than 100 μm [31–33]. The higher frequency employed by ultrasonic activation leads to a more complex pattern of several nodes and antinodes than those of sonic devices. The currently available ultrasonic devices operate at 30 kHz leading to an oscillation pattern of approximately three wavelengths, or six nodes, and antinodes spaced approximately 5 mm apart on the file [33]. The geometry and material properties of the instrument determine the exact oscillation pattern. The oscillation amplitude of the tip of current ultrasonic devices and instruments is on the order of 10–100 μm in the direction of oscillation. There is also a small oscillation perpendicular to the main oscillation direction [32, 33].
The cross-section of instruments available for ultrasonic activation is circular (non-cutting) or square (cutting). The cutting action of the instruments is not needed for this application; however, these files are used for ultrasonic activation for historical reasons. In 1980, Weller [34] proposed intentional wall contact during ultrasonic activation; however, later it was shown that the irrigant streaming is better in the absence of intentional contact [35]. Nevertheless, it was recently demonstrated that unintentional contact with a root canal wall nearly always takes place [36]. The amount of contact depends not only on the power setting used but also on the instrument stiffness and on the force with which the instrument is pushed against the root canal wall. Light contact does not appear to affect its cleaning mechanisms of streaming and cavitation as the file oscillation is not damped out. Instead it builds up a secondary oscillation at audible frequencies during which the file displaces away from the wall and keeps on oscillating at the driving ultrasonic frequency [36].
Heating of the irrigant inside the root canal by the ultrasound is limited to at most 15 °C in 60 min [37].
3.4 Clinical Procedures of Irrigant Activation Techniques
3.4.1 Irrigation Activation Protocols
An easily application of irrigation protocol for sonic, ultrasonic, or laser-activated irrigation is the “intermittent flush technique” first described by Cameron [150]. The irrigant is first delivered into the root canal by syringe irrigation. Then the irrigant can be activated inside the root canal allowing the disruption of the substrate from the root canal wall. After activation, the root canal needs to be rinsed using syringe irrigation in order to remove the substrate loosened from the root canal wall by the irrigant activation.
Another protocol comprises a continuous flow of irrigant through or alongside the handpiece or fiber into the pulp chamber. The irrigant then has to flow from the pulp chamber or coronal root canal to the apical root canal by the activation of the instrument thereby enhancing irrigant delivery into the (apical) root canal.
There are also needles (23–30 gauge) on the market which allow a continuous flow of irrigant through the needle into the root canal during ultrasonic activation of the needle. These needles allow irrigant delivery refreshment and activation at the same time.
For the moment, it seems that irrigation protocols are most effective when the root canal has been shaped with a final apical file because there is more space in the root canal for fluid dynamic effects [45, 55]. However, this does not to imply that other protocols cannot be used or will not be effective during the root canal treatment.
3.4.2 Sonic Activation
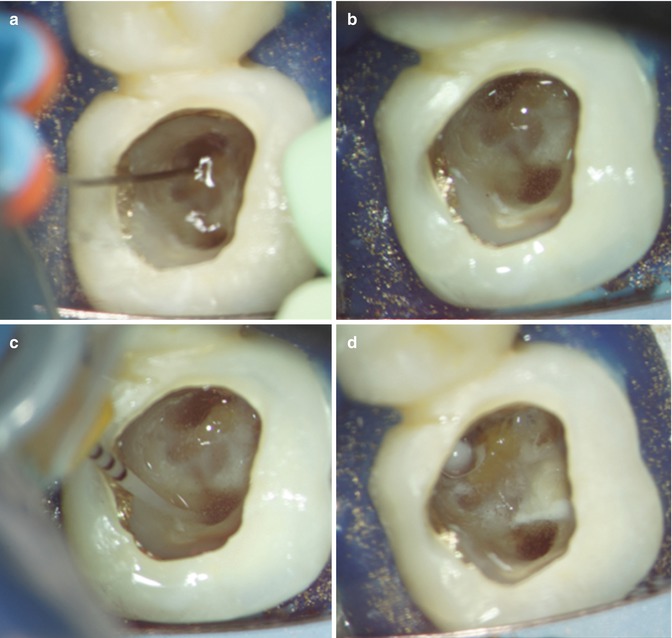
Sonic-activated irrigation can be performed using sonic handpieces that can drive instruments at sonic frequencies (Fig. 3.2). Traditionally only cutting files were available. Today, there are also several new sonic activation systems available on the market like the EndoActivator system or the Vibringe. The EndoActivator system allows a variation in driving power, frequency, and the size of polymer tips that do not cut into the root canal wall. The suggested manufacturer use advises delivery of the irrigant into the root canal by syringe irrigation after creating a “fully tapered shape.” The irrigant is activated for 30–60 s using a pumping action in short 2–3 mm strokes.
Fig. 3.2
(a–d) Sonic activation, effect on NaOCl in the pulp chamber
Vibringe system uses a sonically oscillating needle to deliver the irrigant into the root canal. The Vibringe can be used throughout the complete root canal treatment procedure.
3.4.3 Ultrasonic Activation
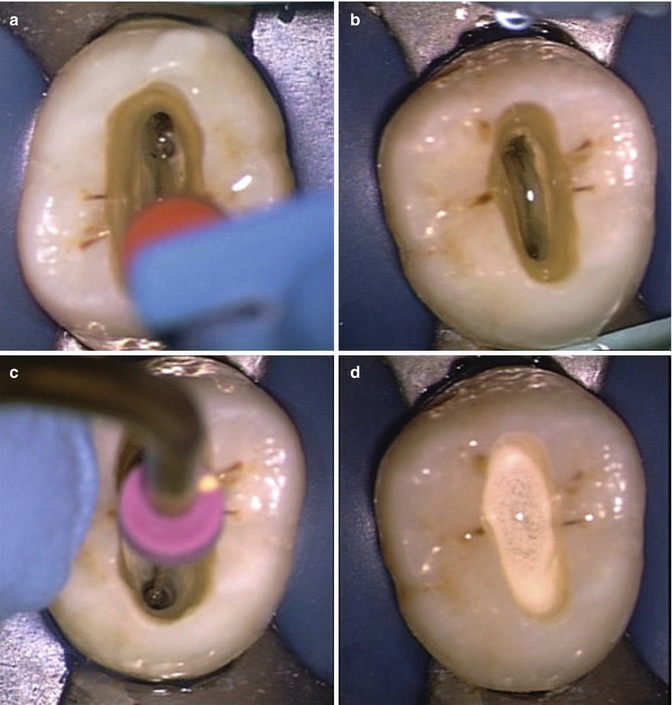
For ultrasonic activation, most of the devices already present in the clinic can be used in combination with a variety of instruments (Fig. 3.3). Occasionally special chucks or irrigation systems are needed. Instruments for all of the mentioned activation protocols are available. The instruments can be applied up to 1–2 mm from working length (with the exception of some of the ultrasonically activated needles) or at the beginning of a strong curvature in order to prevent heavy wall contact [80]. For the “intermittent flush technique,” a sequence of three times 10 s seems to be favorable for dentin debris removal [17]. For a continuous flush, 1 min is advised. For optimal cleaning efficacy of oval extensions, isthmuses, and lateral canals of which the position is known, the instrument should be directed to oscillate towards these areas if possible [76].
Fig. 3.3
(a–d) Ultrasonic activation, effect on NaOCl in the pulp chamber
At the moment, low-intensity settings of the ultrasonic energy are advised to prevent fracture of the instruments. Normally fractured instruments will easily flow out of the root canal. Non-cutting instruments are available which can safely be used in the root canal. Heavy contact of the file with the root canal walls should be avoided [36].
3.4.4 Laser Activation
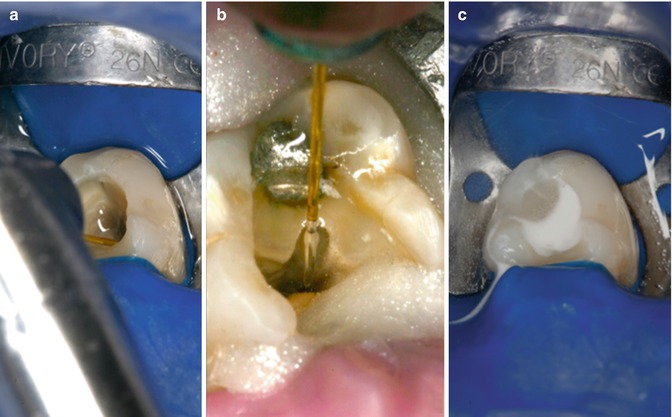
For laser-activated irrigation, Er:YAG or ErCrYSGG laser systems are available on the market. The “intermittent flush technique” or a continuous flow into the pulp chamber can be used. The laser fiber can be inserted 1–2 mm short of working length and vertically moved up and down within the apical third [115]. It can also be placed in the pulp chamber just above the root canal orifice. The latter has been described for conventional fibers [24] and for specially designed fibers (PIPS: photon- induced photoacoustic streaming) (Fig. 3.4) [25, 27].
Fig. 3.4
(a–c) Laser activation, effect on NaOCl in the pulp chamber
Commercially available laser devices allow for a variation of the size and type of optical fibers, pulse repetition frequency (PRF), applied energy, and pulse length. De Groot et al. [115] reported as optimal settings a combination of low power (80 mJ) per pulse and a PRF of 15 Hz. Significant loss of irrigant from the pulp chamber was reported for energy settings higher than 120 mJ per pulse reducing the efficacy of the irrigation procedure.
For the PIPS technique, the recommended energy setting is even lower: 20 mJ. The PIPS fiber is placed at the coronal opening of the root canal after filling the root canal system and pulp chamber with irrigant. There is noticeable irrigant loss during activation therefore a continuous flow of irrigant is required in the pulp chamber during activation. The laser-activated irrigation part will be also treated in depth in Chaps. 9 and 10.
3.5 Flow Characteristics for Different Irrigation Systems
3.5.1 Syringe Irrigation
The characteristics of the flow in the root canal during syringe irrigation depend primarily on the type of needle used [12, 38, 39] (Fig. 3.5). Two needle groups can be distinguished namely closed-ended and open-ended needles. The differentiation is based on the needle outlet type and the resulting flow. Open-ended needles, such as those with a flat, beveled, or notched outlets, generate a jet that extends along the longitudinal axis of the root canal apically to their tip. The irrigant then returns to the coronal opening along the outside of the needle as the apex is considered closed [40, 41]. As the jet is directed at the apical foramen, pressure is developed there with an associated risk on irrigant extrusion [42, 43]. The jet may become unstable and break-up at high flow rates or large distances from the apex [38] leading to unsteady (not turbulent) flow with enhanced mixing and reduced pressure at the apex.
Fig. 3.5
Needle flow. Computational fluid dynamics results for the shear stress (a, c) and flow velocities (b, d) from a side-vented (a, b) or open-ended (c, d) needle inside a root canal (Boutsioukis et al. [47])
In the case of the closed-ended needles (side-vented, double-side-vented), the irrigant leaves the needle from the side outlets and is directed towards the apex under an angle of approximately 30°. The flow then curves around the tip of the needle before it returns to the coronal opening [12, 39, 44]. A series of counter-rotating vortices (flow structures where the fluid is rotating) is formed apically from the tip up to the apex. The size, position, and number of vortices are determined by the needle insertion depth, root canal size, taper, and flow rate. The irrigant velocity inside each consecutive vortex drops rapidly towards the apex resulting in a very low irrigant replacement near the apex. The irrigant exchange of the closed-ended needles is therefore limited to 1 mm beyond the needle tip [12, 38, 39, 44–47] at clinically realistic timescales. A low velocity at the apex is associated with a small pressure, making closed-ended needles safer in terms of risk on irrigant extrusion [42, 43].
For both types of needles, the flow that is created contributes to the cleaning efficacy by replacing and mixing fresh irrigant with irrigant that has been consumed during its reaction with biomaterials in the root canal system. Concurrently with the flow, a shear stress up to 500 N/m [12] is exerted on (the material on) the wall, which is directly proportional to the flow velocity. As the flow from both needle types only dominates a limited area beyond the needle tip, it is important to place the needles close to working length. Closed-ended needles may be placed around 1 mm from WL. For open-ended needles, a larger distance is recommended due to the higher pressure developed apically.
A curved root canal limits the placement of stiff needles near the apex. However, small size (30G or 0.32 mm) flexible irrigation needles are currently available and can facilitate injection near the working length even in severely curved canals provided that the canal is enlarged at least to size 30 or 35. The influence of canal curvature on the flow and the apical pressure is limited [43, 48] except for severely curved canals (Schneider angle 24–28°).
Near the apex, the irrigant flow can be very slow, depending on needle placement and flow rate [12, 38, 45–47], and has even been dubbed as “dead-water” zone or stagnation zone [49, 50]. The flow doesn’t actually stand still there but is too slow to contribute to mixing or to be observed on the time scale of seconds. In addition, the occurrence of a “vapor lock” (bubble entrapment) in the apical part of the root canal has been reported during syringe irrigation of root canals, ex vivo [40, 51] and in vivo [52]. The presence of such a bubble would prevent irrigant from reaching the apical area. A recent study dedicated to this phenomenon has shown that such bubbles could indeed be formed, depending on irrigant flow rate, needle type, insertion depth, and size of the root canal [53]. However, it was also shown (in vitro) that it can easily be removed or prevented by positioning the needle within 1 mm away from working length or by using high flow rates in the order of 0.2 mL/s [53].
The flow pattern of both needles is influenced by the needle size, flow rate, needle insertion depth, horizontal positioning, root canal size, and taper [12, 36, 38, 44–47]. Small-diameter needles seem to be more effective even when positioned at the same depth [54]. Namely, a smaller needle results in an increase of the annulus area available for the reverse flow between the needle and the root canal wall and also increases the possibility for irrigants to mix apically at the tip for closed-ended needles [45, 46].
Several studies have shown that an increase in the preparation size or taper of the root canal results in a more efficient flow in the apical section of the root canal [45, 46, 54–58]. An apical size 30 .06 taper or larger allows irrigant to disperse and mix 2 mm apically to an open-ended needle, although still only 1 mm apically to the tip of a closed-ended needle [46]. The space that is created by preparation in the apical area appears to be important as a minimally tapered root canal preparation (size 60, .02 taper) appears to give a significant advantage over the tapered ones in terms of irrigant dispersion and mixing [46].
The amount of irrigant delivered is determined by the flow rate and duration of irrigation. An increase in the volume of irrigant allows for improved irrigant dispersion, mixing, and chemical effect and has been shown to improve canal cleanliness [59] and irrigant mixing [60–62].
3.5.2 Negative Pressure Irrigation
The aspiration of irrigant induced by the apically placed microcannula of the negative pressure systems creates a flow that resembles the inverse of the flow pattern described above for positive pressure systems. The irrigant is sucked along the cannula towards the apex, meanwhile creating shear stresses on the walls of the root canal [39]. As the microcannula can be placed up to the apex, irrigant mixing at the apex can be achieved [39, 63].
Various negative pressure irrigation systems are available [15]. Since a lot of data on this system is available, we use the EndoVac system for an estimation of the flow velocities and shear stresses. The maximum possible flow rate through the EndoVac microcannula (30G) is determined by the negative pressure and is, under ideal conditions, 0.05 mL/s for an aspiration pressure of 25.4 kPa [64]. The efficacy of the system depends on the magnitude of this pressure which is difficult to assess on the dental unit. The results of various studies are therefore sometimes difficult to relate to clinical practice.
Assuming a root canal of size 40, .04 taper (this is recommended for an optimal flow rate under clinical conditions) [64], an average irrigant velocity of 1.1 m/s can be calculated for the root canal near the tip of the microcannula [65]. At such flow rates, the flow will remain laminar [65]. As the flow velocities produced during positive pressure irrigation (syringe irrigation) are typically higher than this in areas near the needle outlets, negative pressure systems are expected to have a lower shear stress on the root canal walls [39] and therefore be less effective than syringe irrigation regarding cleaning efficacy of the root canal wall. On the other hand, the generation of a two-phase flow (irrigant and bubbles) has been suggested as a mechanism of enhanced cleaning [66]. In vitro tests are as of yet inconclusive on the cleaning efficacy of this technique compared to other techniques [16, 39, 66, 67].
The absence of high apical pressures could make the negative pressure technique safer than positive pressure systems [22, 68]. However, it is difficult to fully control the flow near the apex [16].
3.5.3 Intermezzo: Flow into Lateral Canals and Tubules
The flow generated by positive and negative pressure techniques is predominantly along the wall axis of the main root canal lumen. However, the lateral canals and isthmuses that are part of the root canal system can also harbor biofilm and dentin debris and should be cleaned as well [69]. The absence of a strong lateral flow component in the direction of these root canal extensions leaves many areas of the root canal uncleansed and consequently biofilm could remain. The clinical relevance of this was highlighted by two recently published case reports [69, 70], where a direct correlation between persistent apical periodontitis and a biofilm remaining in a lateral canal or other ramifications was suggested.
The tubules that are present in the dentinal walls of the root canal can be considered an extreme case of these lateral canals. The tubules range from 0.5 to 3.2 μm in diameter but can nevertheless harbor bacteria [71]. Although there is no consensus on the possible clinical effect of these microorganisms on root canal treatment outcome, it seems reasonable to take efforts against them.
When irrigant flows only over the entrance of the lateral canal or tubule, only very limited irrigant enter the lateral canal/tubule [72]. Such a so-called cavity-driven flow is well known for its limited flow in this cavity [73]. It was recently shown that the flow is limited by two times the diameter of the cavity which is a few hundred micrometers for lateral canals but only a few micrometers for tubules [72]. Beyond this distance, irrigant will have to be transported by diffusion which is typically very slow [72, 74].
Irrigant activation/agitation techniques that create a flow in the lateral direction could improve the flow into lateral canals and tubules.
3.5.4 Sonic and Ultrasonic Activation
The sonically or ultrasonically oscillating instruments act as a mixing device when they are agitating the irrigant. The oscillations induce a streaming of the fluid around it, leading to alternating pressures and shear stresses on biological material on the root canal wall [75].
The flow along the file in the axial direction is determined by the pattern of nodes and antinodes that are set up along the instrument. Sonic instruments typically have a single antinode at the tip and a node at the driven end which leads to streaming from the tip to the driven end. The multitude of antinodes and nodes on an ultrasonically driven instrument leads to a more complex pattern of microstreaming along the instrument. In both cases, there is a strong component of the flow in the lateral direction, which is advantageous for cleaning extensions of the root canal (lateral canals, isthmuses, webs, fins, and oval extensions) [51, 76, 77]. Increasing the oscillation amplitude (e.g., a higher intensity of the ultrasound) leads to more effective cleaning [78].
The flow directed towards the apex is weak for both sonic and ultrasonic activations [79]. Mixing and replenishment of irrigant facilitates debris removal beyond the file tip when the ultrasonically activated instrument is inserted 3 mm from the working length [80]. The risk on irrigant extrusion is minor due to the absence of a strong flow towards the apical foramen.
Although sonic or ultrasonic instruments should be placed near working length, the curvature of a root canal may limit the access to the apex for the instrument. Nevertheless, when an instrument is inserted to or near the working length, its oscillation may be affected by heavy contact or binding of the instrument with the root canal wall [81]. Therefore, it is advised to insert the ultrasonically driven instrument just in the beginning of the curvature without bending of the instrument. The flow itself should not be affected by the curvature because the radius of curvature is typically much larger than the scale on which the streaming takes place [80].
3.5.4.1 Acoustic Streaming
Ultrasonic activation leads to a special kind of flow called acoustic streaming. Acoustic streaming is a phenomenon already introduced in 1884 by Lord Rayleigh [82] and extended later to the case of a cylinder oscillating with high amplitude [83] inside another cylinder [84, 85]. The application of acoustic streaming induced by an oscillating cylinder to clean biomaterial off a surface was first described by Williams and Nyborg in 1970 [86, 87].
Acoustic streaming consists of two flows superimposed on each other (Fig. 3.6). One part of the streaming is oscillatory and the other is steady. The strengths of both components depend on the oscillation amplitude of the file. Ahmad and coworkers [88] used the theory of acoustic streaming to describe ultrasonic activation in endodontics; however, only the steady part of the flow was considered. It was shown recently that the oscillatory component can also contribute significantly to the overall streaming [75].
Fig. 3.6
Acoustic streaming. Sketch of the acoustic streaming induced by an ultrasonically oscillating file (black circle in (a)) (Verhaagen et al. [75]). Near the file, there is an area with oscillatory flow; further away and in the direction of oscillation, there is a steady flow in the shape of a jet. This jet is important for cleaning extensions of the root canal. When oscillating the file towards an extension (b), the jet will clean the extension, whereas when oscillating perpendicular to the extension, (c) there is much less flow in the extension (Jiang et al. [76])
The oscillatory part of the acoustic streaming makes the flow oscillate forward and backward together with the file, with a velocity equal to that of the file . However, the velocity decreases quadratically with the distance from the file, and the oscillatory flow component is therefore only important near the file. Due to its oscillatory nature, the fluid exerts an alternating pressure and shear stress on the material on the root canal wall with magnitudes of 100 and 1 kPa, respectively [75]. The values for the pressure and the shear stress are similar to those reported for syringe irrigation at a very high flow rate (0.26 mL/s) near the outlet [44]. For ultrasonic activation, these forces are present around every antinode of the instrument; therefore, more sections of the wall can be cleaned simultaneously. The oscillatory nature of the pressure and the shear stress may furthermore induce fatigue in the substrate material [89].
Nonlinear effects of the fluid lead to steady (i.e., non-oscillatory) streaming in the direction of oscillation [76]. These “jets” have a velocity usgiven by:
where ω is the oscillation frequency, y is the oscillation amplitude, and R is the radius of the file. The jet velocity is typically 1 m/s and increases with increasing amplitude or power setting [78]. Because jets specifically form in the direction of oscillation, the oscillation direction of the file should be taken into account in particular when cleaning oval canals, isthmuses, and lateral canals [76].
Whereas the oscillatory component only made the fluid oscillate back and forth, this steady part of the flow is doing the actual transport and mixing of the fluid. The jets also exert a pressure (1 kPa) and shear stress (10 Pa) onto the wall [75] and even at relatively large distances from the instrument, whereas the velocity of the jet only slowly decreases with increasing distance from the file. Near the file, the steady pressure and shear stress values can be one or two orders of magnitude lower than the oscillatory components. That is to say that further away the components may become similar in strength. The pressure is highest in the center of the jet, while the shear stress is highest off-center at a distance of 0.1 times the distance between the oscillating file and the wall [90, 91]. Although the details of the streaming may change [92], especially near sharp corners, acoustic streaming is induced for all of the cross-sectional designs of the current instruments. A nearby wall or the confinement of a root canal significantly affects the streaming as well.
Oscillation of instruments at sonic frequencies does not lead to acoustic streaming because its frequency and associated oscillatory velocity are too low to lead to these nonlinear effects [29].
3.5.4.2 Cavitation
When an instrument oscillates ultrasonically with high amplitude, transient cavitation may be induced. Cavitation is defined as the growth and fast collapse of a bubble [93, 94] and is associated with surface cleaning [95–97], medical therapy, surface erosion [98, 99], and other mechanical effects [96]. This surface cleaning potential makes cavitation interesting for root canal cleaning. In non-pure water (tap water, distilled water), there are often tiny pockets of entrapped gas (cavitation nuclei) on surfaces of walls or particles from which bubbles can grow followed by a fast collapse (a process called heterogeneous cavitation).
The life cycle of a bubble is determined by the oscillating pressure of the ultrasound. The bubbles can grow when the pressure drops from ambient pressure to below the vapor pressure of the liquid (103 Pa for water) [93]. The typical velocity u necessary to generate this negative pressure ΔP in a liquid of density ρ can be estimated from the Bernoulli relation:
In water, the velocity threshold is around 15 m/s which can be achieved with the current endodontic ultrasonic devices but not with sonic devices [29, 37, 100]. The bubble will collapse when the pressure becomes positive during the ultrasonic cycle. Small bubbles always collapse towards a nearby solid hard wall. Alternatively, during bubble collapse next to a soft wall (like a biofilm covering a wall), the soft material might be pulled from the wall towards the bubble [101]. High-velocity jets (hundreds of meters per second) and shock waves [93, 102] have been reported in the literature during the bubble collapse, and these jets lead locally to pressures on the order of 1 GPa and shear stresses of 1 MPa [98]. These small bubbles may therefore further enhance cleaning of the root canal walls.
Several studies have demonstrated the occurrence of cavitation on or very close to endodontic instruments [78, 103–105]. The bubbles prefer to form near the sharp edges of files with a square cross-section (cutting files) where the velocity and pressure gradients are highest. However, there is still a debate whether cavitation can contribution to cleaning the root canal walls or not [103]. Cavitation is well known for its cleaning ability [95, 96, 106]; however, earlier studies have ruled out cavitation as a significant contribution to root canal cleaning [103, 104]. On the other hand, recent articles with newer ultrasound systems show otherwise [37, 107] even at the lowest power settings [100]. High-speed imaging has revealed that a cloud of cavitation bubbles is generated around the tip of the instrument, and this bubble cloud grows and collapses two times per oscillation cycle. However, the bubble cloud was observed to collapse only onto the file itself and not onto a neighboring wall. Besides the bubble cloud, small single bubbles occur around other antinodes on the instrument which have been demonstrated to be sonochemically active. The amount of generated cavitation is different for each file type. However, in general, non-tapered instruments generate more of the small bubbles than tapered instruments [37] (Fig. 3.7). Irrigants with surface-active properties, such as NaOCl, may affect the bubble formation and collapse and therefore lead to a larger bubble cloud consisting of much smaller bubbles [37]. Finally, a smaller confinement (i.e., a narrower root canal) increases the amount of cavitation even beyond the file towards the apex into lateral canals, isthmuses, and around a curvature [100]. Nevertheless, no proof of their added benefit for root canal cleaning has been presented as of today. Meanwhile, the bubbles (clouds) on the file may affect the generated acoustic streaming [75] and therefore may have a negative impact on cleaning.
Fig. 3.7
Cavitation along file. Cavitation occurring on an IrriSafe 25/21 and a K15/21 during ultrasonic activation. The cavitation is visible as white clouds as they are reflecting light from the side. The location of the cavitation coincides well with antinodes on the files that have large amplitudes, as determined with a numerical model (Verhaagen et al. [33]). On the K15/21 file, there is only a large amplitude at the two nodes near the tip, whereas the antinodes on the IrriSafe 25/21 file all have the same amplitude, leading to cavitation at all antinodes on the file
Bubbles don’t necessarily need to collapse. Gas-filled bubbles (such as in beer) may be stable for a relatively long time (seconds to minutes). The oscillating pressure field induced by the oscillating file can make these stable bubbles oscillate with large amplitude and thereby enhance the streaming, and consequently, the cleaning can be locally significantly [93, 106, 108]. This effect is especially useful when bubbles are located in an otherwise difficult to access area such as lateral canals and isthmuses. This mechanism (stable cavitation) was recently observed near an ultrasonically oscillating endodontic file where a stable cavitation was very effective in removing a layer of viscoelastic hydrogel [109]. In another study, a synergistic effect of a microbubble emulsion and ultrasonic agitation was observed to improve biofilm removal [110].
Only gold members can continue reading. Log In or Register to continue
 . However, the velocity decreases quadratically with the distance from the file, and the oscillatory flow component is therefore only important near the file. Due to its oscillatory nature, the fluid exerts an alternating pressure and shear stress on the material on the root canal wall with magnitudes of 100 and 1 kPa, respectively [75]. The values for the pressure and the shear stress are similar to those reported for syringe irrigation at a very high flow rate (0.26 mL/s) near the outlet [44]. For ultrasonic activation, these forces are present around every antinode of the instrument; therefore, more sections of the wall can be cleaned simultaneously. The oscillatory nature of the pressure and the shear stress may furthermore induce fatigue in the substrate material [89].
. However, the velocity decreases quadratically with the distance from the file, and the oscillatory flow component is therefore only important near the file. Due to its oscillatory nature, the fluid exerts an alternating pressure and shear stress on the material on the root canal wall with magnitudes of 100 and 1 kPa, respectively [75]. The values for the pressure and the shear stress are similar to those reported for syringe irrigation at a very high flow rate (0.26 mL/s) near the outlet [44]. For ultrasonic activation, these forces are present around every antinode of the instrument; therefore, more sections of the wall can be cleaned simultaneously. The oscillatory nature of the pressure and the shear stress may furthermore induce fatigue in the substrate material [89].