Although the problems related to mice date back to ancient times, the modern era began with the invention of the classic mousetrap in the 1890s. ∗
∗ Although it is debated, William C. Hooker of Abingdon, Illinois, is credited with inventing the modern mousetrap in 1894.
It was a simple device consisting of a spring, a metal bar, a wire trip, and some wire fastenings, all embedded into a base to hold them together. It was designed to solve the problem with great efficiency, 1 mouse at a time.
Shortly after its invention, others sought to improve the design through technical advancements with emphasis on safety, efficiency, and outcome. Subsequently, there have been endless variations over the years that followed in identifiable waves of emphasis that shifted from a focus on “mousetrap science” to, at other times, a focus on the science of understanding mice.
In terms of technical advancements, thousands of different mousetraps have been designed over the years, all with differing advantages and disadvantages. There have been devices made of various configurations of plastic and wire; some have involved electricity, and many worked by virtue of adhesives. Along with some of these technological advances, some individuals and even organizations have believed that the methods used were inappropriate for solving the problem of mice. There have been differences of opinion, debates, and even governmental scrutiny of the various mousetraps.
In terms of the scientific knowledge about mice, much has been learned: anatomy, physiology, and psychology have been the main foci of these types of inquiry. As a result, a great amount of information has been produced about how mice can be identified, how they function, how they can be dealt with, and what problems they can cause. Although this is valuable information, the derived scientific knowledge about mice was intended to be relevant to the technology associated with mousetrap design and the successful demise of mice.
So, you are probably wondering by now “what does all this talk about mice and mousetraps have to do with orthodontics?” The answer is “nothing!” The words above, however, are intended to make a point. If you substitute “malocclusion” for “mouse” or “mice,” and “orthodontic appliance” for “mousetrap,” you will note that the history of our specialty is also recounted in a loose reading of the paragraphs above. The point that I am trying to make is that our specialty depends on the advancements in our relevant science about humans as well as our advancements in treating humans clinically, and that they cannot stand on their own if we are to be considered the learned specialty in dentistry called orthodontics as opposed to a craft or a trade.
During this past year, in preparation for the 100th anniversary of the AJO-DO , I realized that I knew very little about the specialty of orthodontics preceding my enrollment in the orthodontic program at Case Western Reserve University in 1973. So to effect some degree of remedy for that lack of knowledge and appreciation, I proceeded to review the Journal from 1915 to 2014. Yes, that is 100 years of the AJO-DO , involving 1209 issues, more than 18,000 articles written by more than 37,000 authors, and approximately 120,000 pages of text. Of course the review consisted of cursory scans, but I will also admit that I stopped to read some articles partially or in their entirety and paused to think about what was important to a particular era. While this type of review does not qualify one to be a historian or an expert, perhaps it does earn a basis from which to offer an opinion.
What, then, has happened over this century of progress? In the beginning years of orthodontics, there was great interest in clinical matters that centered on learning how to use various devices and strategies to correct malocclusion. Of course, there were also fundamental skills (sometimes rudimentary) that needed to be learned, including making and trimming casts, placing bands, soldering, scaling teeth, taking photographs, formulating a diagnosis and a treatment plan, understanding basic biomechanics, setting up an office, and finding ways to work with others (especially general practitioners, pediatric dentists, and oral surgeons). There were also numerous demonstrations of successful treatments and an earnest campaign to provide orthodontic treatment to all those in need.
As to the “science” of orthodontics, in the beginning the focus was not clear. Angle believed that our efforts should be directed toward the science of occlusion; others thought that our efforts and time should be directed toward a better understanding of the etiology of malocclusion. Inquiry in that direction showed interest in the soil used to grow our food, proper nutrition, syndromes, focal lesions of the brain, allergies, habits, postural activities, comparative anatomy, histology, anthropology, endocrines, heredity, genetics, and so on. In this beginning, empiricism was plentiful; strong opinions and strength in debates carried the day.
As time went on, new technologies incited new types of scientific inquiries. A good example of this is the invention of the roentgenographic cephalometer in the late 1920s by B. Holly Broadbent; it is often called the single greatest advancement in orthodontics. This device incited inquiry into facial growth by Broadbent and many others, and assessments of the effects of treatment by Allan Brodie and others. Great interest in understanding, predicting, and eventually controlling facial growth followed.
Still, in those early days, orthodontics was clearly a craft-minded specialty where manual skills were emphasized, and its science was somewhat unfocused. To that point, Byron O. Hughes remarked in 1945 that:
I have stressed the importance of collecting and utilizing facts in planning and carrying out treatment on individuals. I have emphasized the danger of structuring the profession upon ideals, concepts, philosophies, and techniques of treatment. My concluding opinion is that orthodontics has been poorly scienced, and contrarily that, on the whole, it has been practiced well.
Over time, however, study designs changed, and descriptive statistics began to be used to strengthen arguments; there was no inferential testing (eg, t tests) from which successful conclusions could be drawn until the 1950s. But research models and designs continued to improve, new ideas emerged, and advances in technology generated new areas of scientific inquiry and new clinical treatments. Examples are plentiful: new wires, brackets and appliances, adhesives, computers and methods of imaging, implants and miniplates, and many other new opportunities developed. Each step forward was followed by improvements in our clinical options and in our scientific knowledge. A great example was seen with the introduction of direct bonding; the clinical need for appropriate adhesives produced an avalanche of scientific inquiries and publications … and improved adhesives.
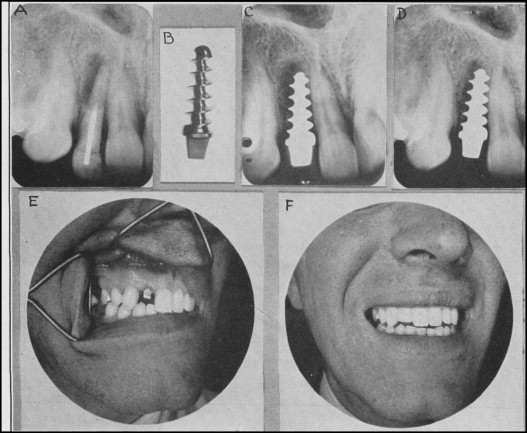
In all of this, I would argue that these advances involved a blend of identified clinical needs, scientific inquiries, and then clinical applications. As an example of this relationship, I will point to an article published in the Journal in 1939 by Alvin Strock. Based on previous research findings, he believed that dental implants failed because of the deleterious nature of the metals used in the implants and the method of insertion of the implants into the alveolus. Subsequently, he developed a Vitallium screw and inserted these screws into the alveolus in dogs and the extraction sites in 3 patients followed by restorations with celluloid crowns ( Fig ). This effort is acknowledged as the first successful placement of a dental implant … ever. By the way, this study was published in the AJO in 1939.