This article updates a simple checklist of foundational knowledge in aesthetic dental concepts that allows clinicians to organize their thoughts, to record the concerns of the patient, and to map out those improvements that must be addressed. This adjunct is called a Smile Evaluation Form. Along with other adjuncts such as radiographs, study casts, and diagnostic wax-ups, the Smile Evaluation Form allows clinicians to form a conceptual visualization of the expected end point. It provides a checklist for discussions with other disciplines in the team, to provide a logical sequence of treatment with a mutually agreed-on end point.
Key points
- •
The Smile Evaluation Form is a simple checklist of foundational knowledge in aesthetic dental concepts that allows clinicians to organize their thoughts, to record in an orderly fashion the concerns of the patient and the patient’s existing problems, and to practically map out those improvements that must be addressed.
- •
On the completion of the Smile Evaluation Form, the clinician generally has a starting point in understanding the patient’s problems, and also an end point of what is needed to be changed in order to provide a predictable aesthetic result for that patient.
- •
Along with other adjuncts, such as radiographs, study casts, and diagnostic wax-ups, the Smile Evaluation Form allows clinicians to form a conceptual visualization of the expected end point.
- •
The Smile Evaluation Form provides a checklist to refer to in discussions with other disciplines in the team, to provide a logical sequence of treatment with a mutually agreed-on end point.
Introduction
In the modern practice of dentistry, it is no longer acceptable to just repair individual teeth. More and more patients are demanding a final appearance that is not only physiologically and mechanically sound but also esthetically pleasing. In addition to restoring and reconstructing the broken-down dentition, bleaching, bonding, and veneering have created possibilities for a wide variety of elective dental treatments for the purposes of enhancing appearance and often reversing the visual signs of aging. The initial consultation visit is extremely important in understanding the chief concerns of the patient and recording as much information as possible to allow the doctor to decide whether it is possible to provide what the patient is looking for. The author has found that, with the help of the Smile Evaluation Form, , the doctor can formulate the patient’s basic problems and can quickly describe to the patient those discrepancies from the norm. The patient has a sense of what needs to be done and the doctor can explain what other adjuncts are needed to complete the best course of treatment. This form has gone a long way to communicating patients’ needs, and patients can more easily decide on accepting the need for radiographs, study casts, and possible diagnostic wax-ups of the expected result.
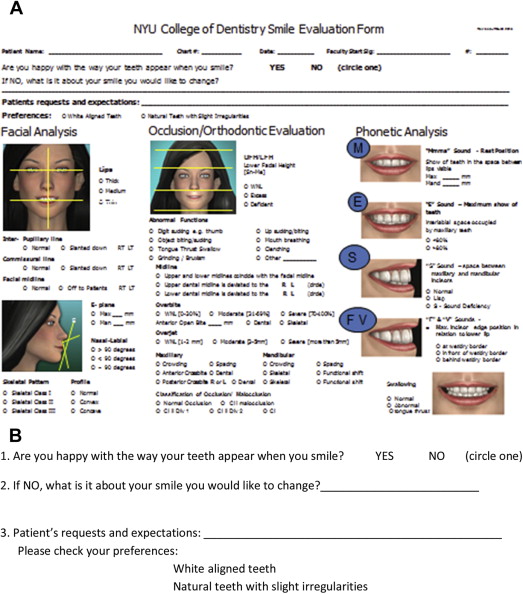
The first part of the form ( Fig. 1 A ) allows patients to indicate whether they are interested in any change to their existing smile. If the answer to this question is yes, then it is left to the patient to describe what their chief concerns might be. Patients may not be able to identify their needs in other than short sentences. It is at this juncture that clinicians must decide whether the expectations of the patient are reasonable and whether the possible treatment needed is within their area of expertise. If the clinician is in doubt about either question, the case should be referred.
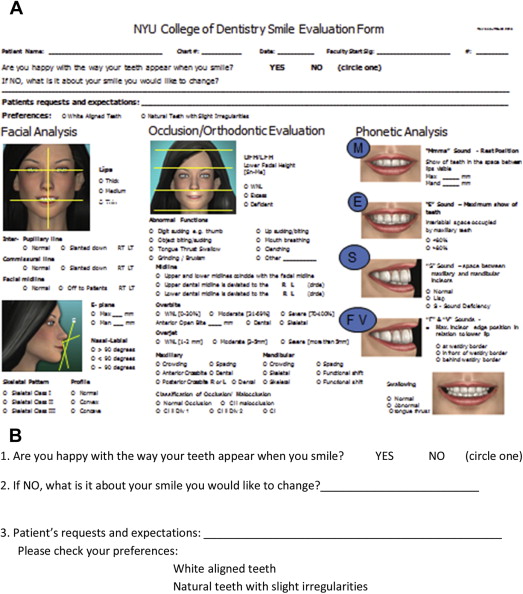
Three simple questions usually give clinicians a good starting point in allowing patients to express their concerns. These questions are found at the top of the updated January 2015 Smile Evaluation Form (see Fig. 1 B).
If the clinician has the experience and ability to meet the patient’s stated expectations or has a team that can provide the best outcome, careful consideration should then be given to the patient entirety.
This consideration must include a thorough evaluation of the:
- 1.
Facial analysis
- 2.
Occlusion/orthodontic evaluation
- 3.
Phonetic analysis, including swallow evaluation
- 4.
Dentofacial analysis
- 5.
Dental analysis, especially in the smile zone
- 6.
Evaluation of the surrounding hard and soft tissue
Each of these components and how they build on one another provide the lattice structure for the finished case.
Dental photography and/or video recording is becoming more and more the standing operating procedure in this initial consultation visit, because it is often necessary to refer back to these photographs and video to establish a final treatment plan.
The standard set of photographs taken for patients is shown in Fig. 2 .
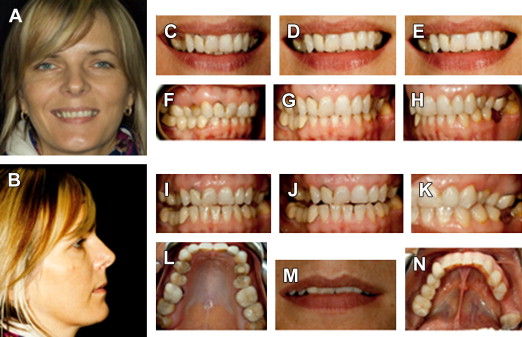
Collecting these photographs (see Fig. 2 ) a clinician can then superimpose their patients’ pictures onto the Smile Evaluation Form. This article now addresses the form so that readers can understand the data collection process and, with practice, may go through the form quickly and accurately. Once accomplished accurately, clinicians can easily glean from this form a good understanding of each patient’s needs.
Introduction
In the modern practice of dentistry, it is no longer acceptable to just repair individual teeth. More and more patients are demanding a final appearance that is not only physiologically and mechanically sound but also esthetically pleasing. In addition to restoring and reconstructing the broken-down dentition, bleaching, bonding, and veneering have created possibilities for a wide variety of elective dental treatments for the purposes of enhancing appearance and often reversing the visual signs of aging. The initial consultation visit is extremely important in understanding the chief concerns of the patient and recording as much information as possible to allow the doctor to decide whether it is possible to provide what the patient is looking for. The author has found that, with the help of the Smile Evaluation Form, , the doctor can formulate the patient’s basic problems and can quickly describe to the patient those discrepancies from the norm. The patient has a sense of what needs to be done and the doctor can explain what other adjuncts are needed to complete the best course of treatment. This form has gone a long way to communicating patients’ needs, and patients can more easily decide on accepting the need for radiographs, study casts, and possible diagnostic wax-ups of the expected result.
The first part of the form ( Fig. 1 A ) allows patients to indicate whether they are interested in any change to their existing smile. If the answer to this question is yes, then it is left to the patient to describe what their chief concerns might be. Patients may not be able to identify their needs in other than short sentences. It is at this juncture that clinicians must decide whether the expectations of the patient are reasonable and whether the possible treatment needed is within their area of expertise. If the clinician is in doubt about either question, the case should be referred.
Three simple questions usually give clinicians a good starting point in allowing patients to express their concerns. These questions are found at the top of the updated January 2015 Smile Evaluation Form (see Fig. 1 B).
If the clinician has the experience and ability to meet the patient’s stated expectations or has a team that can provide the best outcome, careful consideration should then be given to the patient entirety.
This consideration must include a thorough evaluation of the:
- 1.
Facial analysis
- 2.
Occlusion/orthodontic evaluation
- 3.
Phonetic analysis, including swallow evaluation
- 4.
Dentofacial analysis
- 5.
Dental analysis, especially in the smile zone
- 6.
Evaluation of the surrounding hard and soft tissue
Each of these components and how they build on one another provide the lattice structure for the finished case.
Dental photography and/or video recording is becoming more and more the standing operating procedure in this initial consultation visit, because it is often necessary to refer back to these photographs and video to establish a final treatment plan.
The standard set of photographs taken for patients is shown in Fig. 2 .
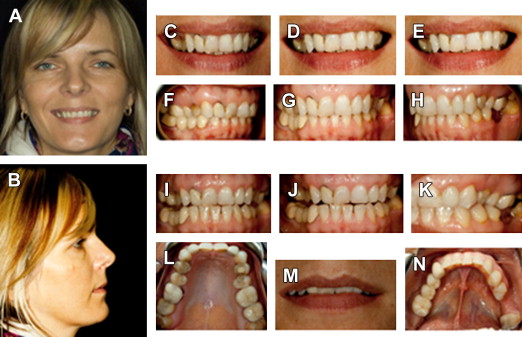
Collecting these photographs (see Fig. 2 ) a clinician can then superimpose their patients’ pictures onto the Smile Evaluation Form. This article now addresses the form so that readers can understand the data collection process and, with practice, may go through the form quickly and accurately. Once accomplished accurately, clinicians can easily glean from this form a good understanding of each patient’s needs.
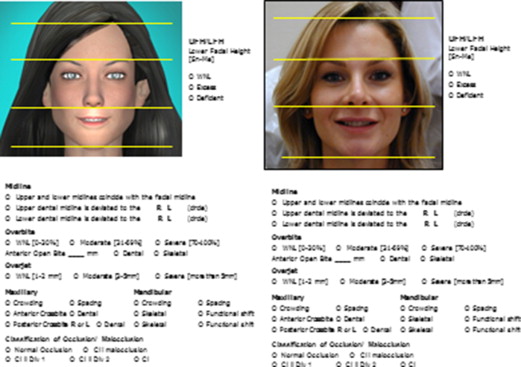
Facial analysis
Frontal View
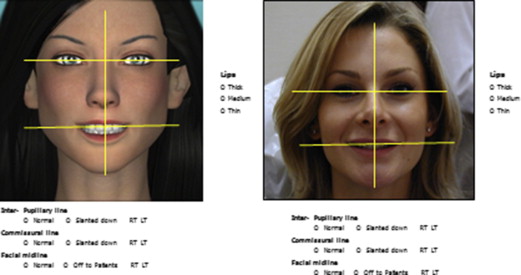
Facial analysis is checked at a conversational distance. The clinician should visualize and if possible record a series of vertical and horizontal lines to evaluate the existing symmetry of the patient’s face. This record will eventually be used to determine the relationship of the patient’s face and dentition in space.
The first yellow horizontal line from the top of the figure is called the interpupillary line. It passes through the center of the pupil of each eye ( Fig. 3 ). The horizontal line below this is called the commissural line. It passes through the corners of the mouth where the upper and lower lips meet. These lines should normally be parallel to one another and are normally parallel to the anterior dental incisal plane. These landmarks are extremely important in the work of Coachman and Calamita and are used in the new concept of digital dental design. The thickness of the upper and lower lips should be quantified and the patient should be asked about past or planned future lip enhancements or reductions. This information should be noted and referred back to in the future.
The vertical yellow line drawn through the glabella (centered between the eyebrows), the tip of the nose, through the center of the philtrum (just under the nose), through the center of Cupid’s bow (the maxillary-facial border of the upper lip), and then to the center of the chin is called the facial midline. This vertical line is important in determining the amount of symmetry in the face. It is generally thought that the more symmetry that exists between the right and left sides of the face, the closer to perfection is the face. Although this perameter is often looked for in professional models, no individuals have a perfectly symmetric face and very few individuals have a face that has close to perfect symmetry. Most dental patients have mild to moderate asymmetry and clinicians should recognize this because it may be necessary to consider this factor in planning the finished restorations ( Figs. 4–7 ).

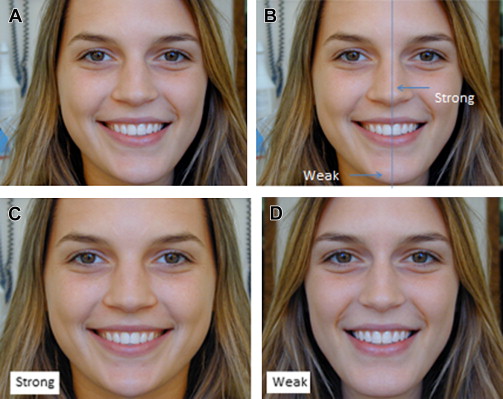
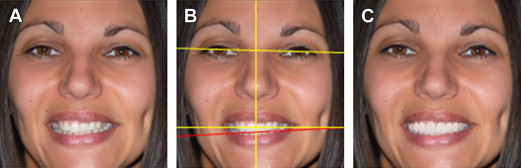
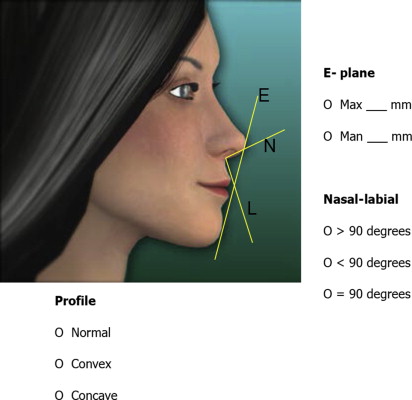
Fig. 7 shows an important imaginary line called the Ricketts E plane. This line, which is drawn from the tip of the nose to the tip of the chin, allows the profile of the patient to be evaluated by comparing the distance from the upper lip to the plane and then the lower lip to the plane. For white men and women, a normal profile has the maxillary lip approximately 2 times the distance to the Ricketts E plane (4 mm) as the lower lip. A concave profile may call for a more prominent position of the maxillary anterior teeth when restoring, whereas a more convex profile may require a less prominent position of the final restorations. Another landmark is called the nasal-labial line angle. Men generally have a 90° to 95° n/l angle, whereas women generally have a 100° to 105° n/l angle.
In Fig. 8 the face is divided horizontally into 3 almost equal portions. The topmost portion runs from the hairline to the top of the patient’s eyebrows. The second portion runs from the eyebrows to the tip of the nose. The lower portion runs from the tip of the nose to the tip of the chin. This third portion is generally slightly wider than the other two portions in a youthful patient with no occlusal wear and a normal vertical dimension. However, this portion might shrink with age and severe wear (posterior bite collapse).