When patients seek cosmetic dentistry, their main concern is how their new smile is going to appear. In trying to achieve a patient’s desire for a more beautiful smile, a careful and comprehensive analysis must be completed to insure the desired outcome is achievable and will function for many years to come. The clinician’s primary goal is to restore the patient’s dentition to ideal form and function. Full mouth rehabilitations need to be done in a systematic way to ensure all the parameters of an esthetic and functional outcome are achieved.
Key points
- •
When patients seek cosmetic dentistry, their main concern is how their new smile is going to appear.
- •
In trying to achieve a patient’s desire for a more beautiful smile, a careful and comprehensive analysis must be completed to insure the desired outcome is achievable and will function for many years to come.
- •
The clinician’s primary goal is to restore the patient’s dentition to ideal form and function. Starting with the smile design process, the ideal upper central incisal edge position should be determined relative to maxillary lip.
- •
Once the ideal upper central incisal edge position is found, the remaining anterior teeth can be positioned and become the determinates for the posterior restorations.
- •
The posterior teeth and occlusion can be worked out to establish immediate posterior disclusion in lateral excursions.
- •
The restorations placed will provide years of service as long as function is incorporated into their design.
- •
Full mouth rehabilitations need to be done in a systematic way to ensure all the parameters of an esthetic and functional outcome are achieved.
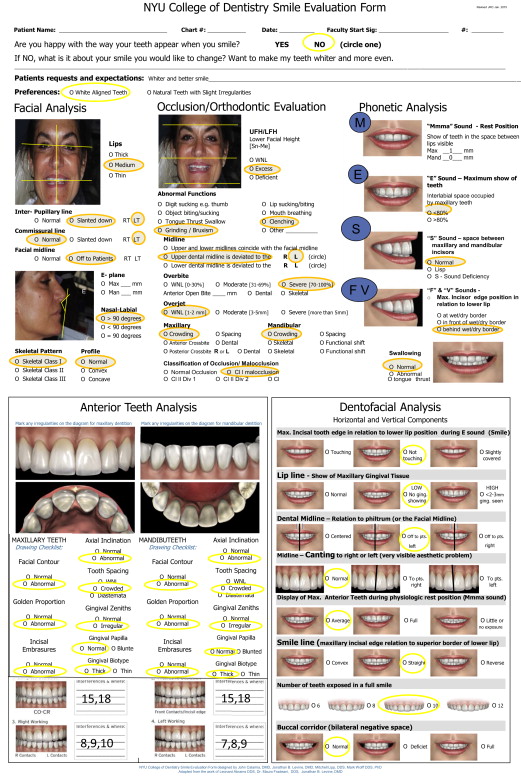
Smile evaluation (see initial form)
It was noted that the patient had severe wear, combined with incisal edge chipping, in addition to an uneven smile line ( Figs. 1–3 ). The anterior teeth were too square and not in an ideal width-to-length proportion. The posterior teeth were worn, and canine guidance needed to be re-established. The gingival zeniths of the central incisors were not in an ideal position. The patient has a low lip line that is not reveal these gingival zenith discrepancies, so the goal of treatment was to try to make the gingival zeniths more favorable without the need for osseous crown lengthening. Even though the gingival zeniths did not show, it was necessary to alter them as much as possible to help the technician create a proper emergence profile and contour in the final restorations. Material selection would be critical in this case. Strength as well as esthetics was necessary. Material choices included full gold, porcelain fused to metal, zirconium, or lithium disilicate. The patient expressed a desire for esthetic restorations. E-Max lithium disilicate (Ivoclar/Vivadent, Amherst, NY, USA) restorations were chosen because of their strength and esthetic properties. To establish the goals, the authors outlined that a full mouth rehabilitation was necessary with a systematic approach.


Diagnostic aids
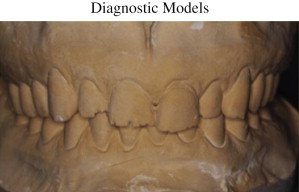
Study Casts
Two sets of diagnostic casts were obtained. One set was used to establish the treatment plan and to have a record of the patient’s original condition. The second set was sent to the laboratory with instructions for the diagnostic wax-up. The prescription to the laboratory must be detailed. The midline, upper central incisor desired length and width, and any gingival recontouring need to be conveyed to the laboratory technician.
Diagnostic wax-up
When performing a full mouth rehabilitation, it is imperative to establish where the anterior teeth need to be first and then restore the posterior teeth to allow function. Anterior guidance with posterior disclusion in lateral excursions will prevent the restorations from failing prematurely. Using smile design principles, it is necessary to determine where the incisal edge of the central incisors should be located. This determination can be done in the mouth with a composite mockup, digitally using photos and a calibrated ruler, or by measuring directly on the patient. Once the incisal edge position is determined, the ideal width-to-length ratio of the central incisor (approximately 80%) can be ascertained. Using the principles of the Golden Proportion, the rest of the anterior teeth can be waxed. Study models ( Figs. 4–6 ) of the patient with a centric relation (CR) bite, using bimanual manipulation, was sent to the laboratory. The prescription to the laboratory indicated the need to lengthen the central incisors by 3 mm. The vertical dimension would need to be opened posteriorly approximately 1 mm to achieve this. The diagnostic wax-up ( Figs. 7–9 ) serves as a template to re-establish the patient’s occlusion and anterior teeth. Ideal forms are established in wax and can be altered and adjusted in the patient’s mouth.


Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


