The central giant cell granuloma is felt to be a benign lesion that only occurs in the jaws, though similar lesions occur in the fingers and toes. Its relationship to the giant cell tumor of the long bones is unknown, but it is felt that the giant cell tumor represents a more aggressive and possibly malignant lesion that rarely occurs in the jaws, if at all. Other authorities feel that these lesions represent a spectrum of disease from malignant to very benign. Central giant cell granulomas normally occur in the anterior part of the jaws (in areas where deciduous teeth were present) and normally occur in the second and third decades, although they have been noted in all decades of life. Histologically similar, or even identical, appearances may occur in hyperparathyroidism, cherubism, and aneurysmal bone cysts, which should normally be ruled out prior to establishing the diagnosis.
When the central giant cell granuloma was first identified as a distinct lesion (previously, it had been included in a group of lesions called “osteitis fibrosa cystica”), it was termed the reparative giant cell granuloma because it was felt to be a self-limiting lesion that would even heal. It is difficult to ascertain the evidence on which this was based, but most authorities now feel that this is not a self-healing lesion and that it will progress if untreated. Worth, however, in the last edition of his textbook on radiology, followed a number of histologically proven central giant cell lesions of the jaws radiographically for many years with no other treatment than the biopsy, and he did show radiographically that some lesions did resolve. The author of this chapter was also able to personally discuss this finding with Dr. Worth in 1978, when he did confirm that this had occurred.
The conventional treatment for the central giant cell granuloma is to establish the diagnosis histologically and to treat the lesions with aggressive curettage. This is associated, however, with a recurrence rate of about 20%, and some authorities feel that there is a more aggressive variant of this lesion, although all attempts to identify this histologically have been unsuccessful to date. However, because of this recurrence rate, and even possible spontaneous regression, alternative treatments have been suggested in an effort to either lower the recurrence rate or to avoid removal or damage to adjacent teeth, soft tissues, or the inferior alveolar and related nerves.
Alternative Medical Treatments
Intralesional Steroid Injection
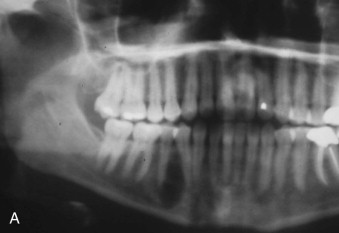
Intralesional steroid injection, an alternative treatment for the management of central giant cell granuloma, was first suggested in 1988. The rationale at that time was that histologically these lesions have a superficial resemblance to the lesions of sarcoid, and because steroids are an effective treatment for sarcoid lesions, they were tried for the central giant cell granuloma. The protocol involves six injections with a 50% mixture of local anesthetic and triamcinolone 10 mg/mL at weekly intervals for six weeks. The protocol suggests the use of 2 cc of this solution for every 1 cc of lesion visible on a Panorex radiograph. There are several reports in the literature on this technique, and most report variable success. There are definitely cases in which this treatment has caused total resolution of the lesion, and even hypercalcification of the lesion as shown in Figure 51-1 , but most authorities report about a 50% success rate. Most practitioners have examples of lesions that either stopped growing in size or partially calcified but still require curettage for the lesion as definitive treatment. It is possible that this treatment is more effective for smaller, unilocular, well-circumscribed lesions where the steroids can enter all parts of the lesion, rather than multilocular lesions where areas may be missed by the steroid injections.

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


