The use of bonded orthodontic molar tubes is becoming more prevalent in orthodontics because they have some advantages over conventional bonding. However, a bonded apparatus can become detached, leading to complications. This article presents the case of a submandibular-space abscess associated with a molar tube that detached during orthognathic surgery and became embedded in the soft tissues. The site became infected, and antibiotics were prescribed. Eventually, the molar tube migrated and could be removed under local anesthesia.
Bonded orthodontic molar tubes are often used because they have some advantages over conventional bonding, such as eliminating the need for orthodontic separation and subsequent cementation of bands, and better periodontal healing. Although these advantages indicate their use in patients requiring conventional orthodontics, bonded molar tubes should not be placed on terminal molars in patients undergoing orthognathic surgery because of the risk of detachment during surgery and the ensuing complications, including contamination and airway obstruction. This report presents a case of submandibular-space abscess after orthognathic surgery caused by a bonded molar tube lost during the surgery.
Case report
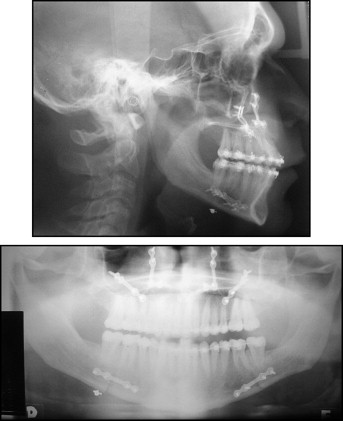
The patient, a 21-year-old man, was referred for surgical treatment of a skeletal Class III malocclusion with maxillary deficiency and mandibular prognathism. After orthodontic preparation, a bimaxillary surgical procedure was planned and performed. The procedure was completed without incident, and the patient was discharged from the hospital 2 days later. After 1 week, when the patient returned for a checkup, lateral and panoramic x-rays were taken. They showed a metallic artifact at the level of the inferior border of the mandible; it was compatible with an orthodontic bracket inside the soft tissues ( Fig 1 ). Intraoral inspection confirmed the absence of the bonded tube on the maxillary second molar. There were no signs or symptoms of infection; we informed the patient, but because of intense postoperative swelling and limited mouth opening, no attempt was made to retrieve the appliance.
After 2 months without complications, the patient reported that “a painful yellowish tumor” had formed below the mandible. Because he lived in another city, we instructed him to seek an evaluation from a local oral and maxillofacial treatment provider as soon as possible. The next day, he phoned to let us know that he had been diagnosed as having a submandibular-space infection; intravenous antibiotics were prescribed, and the site was drained.
Ten days later, he returned to our clinic in Fortaleza, Ceará, Brazil, for examination. Mild swelling was observed in the mandibular region, with a small amount of secretion draining from the surgical site ( Fig 2 ). Occlusion was normal, and no mobility of bone fragments was noted. A panoramic x-ray showed that the previously noted metallic artifact had migrated downward to a position compatible with the extraoral swelling. Under local anesthesia, an incision was made at the previous drainage site; after divulsion with hemostatic forceps, the orthodontic molar tube was identified in the subcutaneous tissue and removed with the forceps ( Fig 3 ). After this procedure, the patient progressed well, with no further signs or symptoms of infection.



