The aim of this article was to describe the Sturge-Weber syndrome in a patient with orthodontic requirements. Pathologies involved in this syndrome affect facial cranial growth.
Sturge-Weber syndrome, also known as encephalotrigeminal angiomatosis or encephalofacial angiomatosis, is a rare, nonhereditary, congenital development, characterized by hamartomatous proliferations of vascular cells that involve the tissues of the brain and face.
It is believed that Sturge-Weber syndrome results from a developmental defect in the first months of gestation, represented by the persistence of a vascular plexus around the cephalic portion of the neural tube. This plexus develops in the sixth week of intrauterine life but normally undergoes regression during the ninth week. The association between cerebral angiomatosis and facial nevus, characteristic of the syndrome, is attributed to the development of the skin of the face from the ectoderm that covers this vascular plexus.
According to Roach, Sturge-Weber syndrome is classified into 3 types. Type I presents facial and leptomeningeal angiomas and glaucoma. Intercranial angioma can be confirmed by histologic examination or typical radiographic findings. Epileptic convulsions or encephalographic alterations allow a presumptive diagnosis in the child with typical nevus. Type II exhibits facial angioma and glaucoma, without evidence of intercranial disease. Type III, which is rare, is characterized by isolated leptomengingeal angioma and absence of glaucoma.
Clinically, a patient with Sturge-Weber syndrome has a port-wine stain, or nevus flammeus, which can be flat or slightly elevated, distributed along the first branch of the trigeminal nerve (ophthalmic), with or without involvement of the other 2 branches (maxillary and mandibular). Abnormalities in the central nervous system, such as cerebral atrophy, leptomeningeal angiomas, and cortical calcifications also form part of the syndrome. Such disturbances can lead to convulsions, mental retardation, and hemiparesia or hemiplegia on the side opposite the nevus flammeus.
The treatment and prognosis of Sturge-Weber syndrome depend on the nature and intensity of the clinical characteristics. Patients with nevus flammeus can be treated with laser therapy; in some, surgical removal of the meningeal angiomatous lesions might be necessary.
The aim of this article was to describe the clinical case of an orthodontic patient with Sturge-Weber syndrome, with neurologic, ophthalmic, facial, and oral involvement; orthodontic considerations are emphasized.
Clinical case
The patient, a boy aged 9 years 6 months, came to the office in Vitória da Conquista, Bahia, Brazil, for orthodontic treatment, with the main complaint of crooked teeth and difficulty in chewing food ( Figs 1 and 2 ). His mother related that he was born with a problem in the left eye, which was diagnosed as congenital glaucoma at the time. According to her, he was never able to see with this eye. She was asked about the stain on the left side of the face and said that she had been told that it was a hemangioma. She related no other complications.

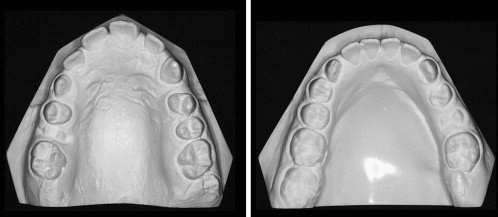
In the clinical examination, an irregular eruptive pattern was noted between the left and right sides; the teeth on the left (affected side) were more developed, with the eruption of permanent teeth including the second molars. The teeth on the right side were at a stage of eruption compatible with the patient’s chronologic age.
In an intrabuccal front view, the occlusal plane had an accentuated deviation as a result of the accelerated maxillary alveolar bone growth on the left side. The superior midline had an accentuated deviation.
Starting with the information collected during anamnesis and the clinical examination, the patient was referred to a dermatologist and a radiologist for diagnosis of the pathologies involved. Periapical, cephalometric, and panoramic radiographs and tomography of the cranium and face were requested ( Fig 3 ).
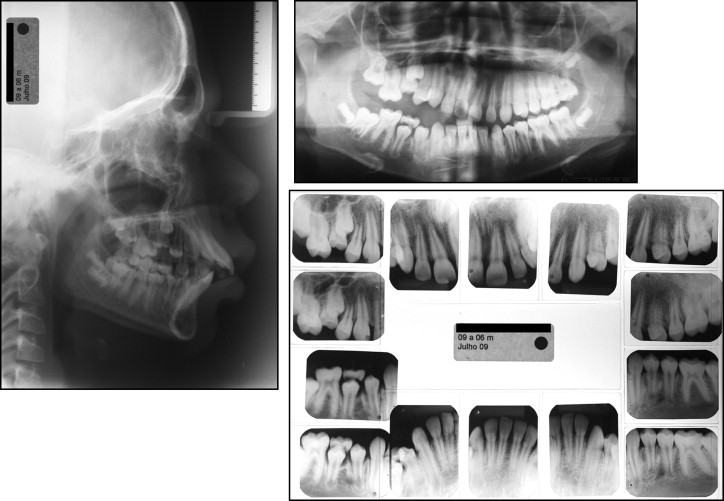
The panoramic and periapical radiographs showed an irregular pattern of development between the left and right sides. The dental elements on the left side were all erupted and had closed root apices. On the right side, the dentition was in the mixed stage with some deciduous and some permanent teeth, with open root apices. The bones also differed between the right and left sides. The alveolar process on the left side was more developed, with more mineralized and mature bone tissue when compared with the right side.
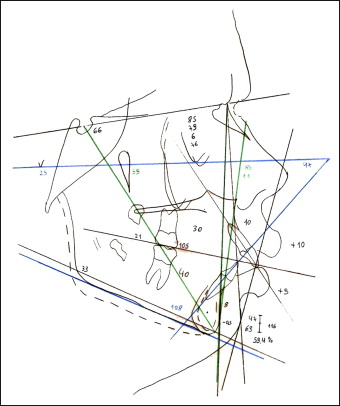
Cephalometric analysis showed a skeletal Class II pattern (ANB, 6°) with deficient mandibular growth (SNB, 79°; SND, 76°), a convex profile (LS-S, +10; LI-S, +9 mm), and a horizontal facial growth pattern (SNGOGN, 33°). With regard to the dental pattern, the incisors were projected and vestibularized (1.NA, 30°; 1-NA, 10 mm; 1.NB, 40°; 1-NB, 8 mm) ( Fig 4 ).
The computerized tomography images of the cranium in the axial plane showed irregular linear cortical calcifications along the spirals of the left occipital and parietal lobes, and a discrete volumetric reduction in these cerebral spirals was noted when compared with the contralateral spirals. After endovenous injection of iodinated contrast, a more pronounced highlight of the left choroid plexus was noted when compared with the right ( Fig 5 ).

In the clinical examination, the patient had a Class II malocclusion with open bite on the right side, superior midline with a 4-mm deviation to the right, and an occlusal plane with a marked inclination. The alveolar mucosa on the right side had a redder color (nevus flammeus). The maxillary arch had a parabolic shape and was slightly contracted, and the mandibular arch also had a parabolic shape.
The patient’s port-wine stain was notable; it was slightly elevated on the left side of the face, extending from the cervical region to the scalp, with greater evidence in the middle and superior regions. The left eye was affected by glaucoma. On the right side, a convex profile was especially apparent, with anteroposterior mandibular deficiency.
From the radiographic, tomographic, and clinical evaluations made by the orthodontist, dermatologist, and radiologist, the diagnosis of Sturge-Weber syndrome was reached.
Discussion
The aim of this article was to report a clinical case of a patient with Sturge-Weber syndrome who sought orthodontic treatment. When seeking orthodontic treatment, the patient and mother did not know that a syndrome was involved, only that he had isolated problems in the eye and hemangioma in the face. When the patient was examined, it was thought that Sturge-Weber syndrome was involved because the classic form of the syndrome includes a port-wine stain and congenital glaucoma. To prove that it really was a port-wine stain and not merely a facial hemangioma, the patient was referred to a dermatologist for evaluation. The dermatologist confirmed that the facial lesion was a port-wine stain and that there were strong indications that Sturge-Weber syndrome was involved.
Although the port-wine stain is not an essential condition of the syndrome, it is the most frequent finding, generally present from birth and affecting half the face; it can extend up to the neck, with characteristic darkening with age: red at first and becoming more purple over time. Only those with nevus flammeus along the ophthalmic ramus develop the syndrome in its classic form. This information was compatible with the findings for this patient.
To finalize the diagnosis, computerized tomography of the cranium was requested to evaluate cerebral involvement, since the mother reported that the patient had never had a convulsive crisis or a learning deficiency.
The tomographic images showed irregular linear cortical calcifications along the spirals of the left occipital and parietal lobes, and a discrete volumetric reduction in the cerebral spirals was noted when compared with the contralateral spirals. After endovenous injection of iodinated contrast, a more pronounced highlight of the left choroid plexus was noted when compared with the right. These findings confirmed the diagnosis of Sturge-Weber syndrome. The absence of both convulsions and learning deficit were compatible with the tomographic images, which showed that involvement was present but discrete. This condition is rare. In the other clinical cases of Sturge-Weber syndrome in the literature, the intracranial manifestations were more evident, compromising the patients’ learning abilities.
Based on the clinical and tomographic findings, the diagnosis of Sturge-Weber syndrome was made. Sturge-Weber syndrome has neurologic manifestations (cerebral anomalies), and cutaneous, ocular, and oral anomalies, which may or may not be associated; nevertheless, the most evident clinical manifestation is nevus flammeus in the face or port-wine stain, which normally follows the trajectory of the V1 and V2 branches of the trigeminal nerve.
There are oral manifestations in approximately 38% of patients that can include hemangiomatous lesions in the lip, oral mucosa, gingiva, tongue, and palatine region. They are generally unilateral and terminate abruptly at the midline. Ipsilateral gingival hyperplasia is observed, characterized by an increase in the vascular component and gingival hemorrhage at the least traumatism. The accumulation of food and the presence of bacterial plaque can intensify gingival inflammation and hyperplasia.
Macroglossia and hypertrophy of the maxillary bone, found in some patients, might result in malocclusion and facial asymmetry.
Dentists must be on the lookout for this syndrome, because traumatic surgical interventions in the region could result in hemorrhages that are difficult to resolve. Moreover, surgical excision of the gingival hyperplasias is not always the procedure of choice, since anticonvulsant drugs might determine the maintenance and recurrence of the lesions.
When we examined the oral cavity of this patient, we noted that the nevus flammeus was also present, which would require a series of precautions before the start of orthodontic treatment. Because it involved a vascular lesion, the tissues had greater susceptibility to hemorrhages; therefore, any procedure involving blood in this region could set off a hemorrhage that would be difficult to resolve. Orthodontic procedures that should be avoided include placement of mini-implants, orthognathic surgery, and extractions. This patient had an accentuated inclination of the occlusal plane. If he had sought treatment as an adult, the resolution would be more difficult because mini-implants or orthognathic surgery would be needed. But alternative and conservative mechanics were available for this adolescent patient, such as the placement of a unilateral left bite-block, with the goal of restricting growth of the alveolar process on the affected side, allowing the other side to develop normally.
Another occlusal problem noted was the skeletal Class II relationship. An extraoral appliance with combined pull to restrict maxillary growth while mandibular growth occurs could be used to correct the Class II relationship. Associated with the orthopedic effect, the dental effect is achieved with distalization of the molars, gaining space in the maxillary arch to improve the biprotrusion and convex facial profile, and correct the superior midline, all at the expense of replacement of the incisors.
The posterior crossbite could be corrected with palatal disjunction. In this patient, the screw would be activated only once every 2 days. This care would help to prevent rupture of small blood vessels on the affected side that might have invaded the palatine suture region.
Although gingival hyperplasia is common in patients with this syndrome, this was not seen in the patient, and we believe that this was because he did not use anticonvulsant medications.
The absence of greater cerebral compromise helps in orthodontic treatment, since it is necessary to have cooperation for auxiliary orthodontic appliances and oral hygiene.
With regard to the facial nevus flammeus, the orthodontist could do little; this deformity must be treated by a dermatologist, with the preferred treatment based on laser therapy.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


