Introduction
The long-term stability of posterior crossbite correction in the mixed dentition has not been sufficiently evaluated. Our aim was to compare long-term outcomes in patients with crossbite correction by using matched controls with normal occlusion.
Methods
After 35 patients were treated for crossbite with a quad-helix or an expansion plate, we used randomized controlled trial methodology to follow them for 3 years posttreatment. All had fulfilled our pretreatment criteria: mixed dentition, unilateral posterior crossbite, no sucking habits, and no previous orthodontic treatment. Transverse relationships, maxillary and mandibular widths, overbite, overjet, arch lengths, and midlines were registered on the study models immediately before and after treatment and at the follow-up 3 years after treatment. The matched control group comprised 20 subjects with normal occlusion and was compared with the first and last registrations for the treated groups.
Results
At follow-up, changes in the treatment groups were equal and stable. The changes were comparable with the control group. All other changes were minor and had no clinical implications. The long-term effect of crossbite correction on midline deviation was unpredictable.
Conclusions
If crossbite is successfully corrected by the quad-helix appliance or the expansion plate, similar long-term stability is achieved. However, in treated patients, mean maxillary widths never reached those of normal control subjects.
Posterior crossbite is a common malocclusion in the deciduous and mixed dentitions, with prevalence rates of 7.5% to 22%. It has been claimed that unilateral posterior crossbite should be treated early to prevent negative long-term effects on growth and development of the teeth and jaws, such as disturbance of temporal and masseter muscle activity in children and increased risk of craniomandibular disorders in adolescents.
Two approaches for correction of posterior crossbite are rapid maxillary expansion and slow expansion, with a quad-helix appliance or a removable expansion plate. Two recent systematic reviews concluded that there is inadequate evidence in support of any method of crossbite correction in the mixed dentition, with a need for additional randomized clinical trials (RCTs). There is only 1 published RCT comparing and evaluating the effectiveness of different treatment strategies for crossbite correction in the mixed dentition. It was a short-term study and clearly demonstrated that the quad-helix appliance was superior to the expansion plate.
The basic goal of orthodontic treatment is to produce a normal occlusion that is morphologically stable and functionally and esthetically well adjusted. However, treatment outcomes vary, depending on the type and severity of malocclusion, treatment approach and timing, patient compliance and growth, and adaptability of the hard and soft tissues. Follow-up studies of treated patients have shown that, although normal occlusion and dental alignment have been achieved, there is a tendency for posttreatment relapse. Crossbite correction is undertaken in the growing child: hence, posttreatment changes must be evaluated in the context of changes associated with normal growth in children who have had no orthodontic treatment. It is therefore appropriate and advisable to use control groups with normal occlusion.
There are few published studies of the long-term effects of crossbite correction and only 1 comparing the expansion-plate and the quad-helix methods.
Our aims in this study were, using RCT methodology, to compare and evaluate the long-term stability in patients who had crossbite correction with quad-helix appliances and expansion plates, with a matched control group with normal occlusion. It was hypothesized that the 2 treatment methods achieve similar changes of a magnitude comparable with those in subjects with normal occlusion.
Material and methods
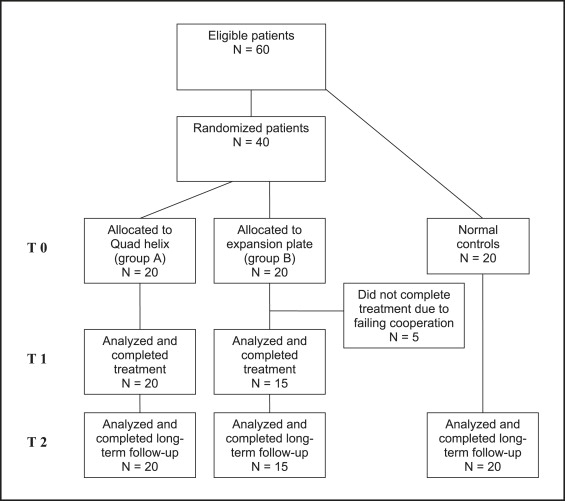
Originally, the study comprised 60 subjects (33 girls, 27 boys): 40 with unilateral posterior crossbite and 20 controls with normal occlusion. All patients were informed of the purpose of the trial and were required to give written, informed consent before enrollment.
Twenty of the crossbite patients had been treated with quad-helix appliances and 20 with expansion plates. Most (n = 30) of the crossbite patients were recruited from an RCT study. Five patients in the expansion-plate group failed to complete the study because of noncompliance and were excluded from the long-term follow-up. The patient flow is illustrated in Figure 1 . Sample size, sex, and age distribution of the subjects are given in Table I . Consequently, the follow-up study comprised 55 patients (30 girls, 25 boys).
| Quad-helix group (n = 20) | Expansion-plate group (n = 15) | Normal group (n = 20) | ||||
|---|---|---|---|---|---|---|
| 11 girls, 9 boys | 10 girls, 5 boys | 9 girls, 11 boys | ||||
| Mean | SD | Mean | SD | Mean | SD | |
| T0 | 9.0 | 1.19 | 8.5 | 1.02 | 8.8 | 0.5 |
| T1 | 10.5 | 1.31 | 10.2 | 1.11 | x | x |
| T2 | 13.8 | 2.0 | 13.1 | 1.29 | 13.9 | 1.59 |
All crossbite patients were consecutively recruited from 2 public dental clinics in the province of Scania, Sweden, and from the Department of General Dentistry, Faculty of Odontology, Malmö University, Malmö, Sweden, from 2001 through 2006. The patients met the following inclusion criteria: mixed dentition (all incisors and first molars in occlusion), unilateral posterior crossbite, no sucking habits or sucking habit discontinued at least 1 year before the trial, and no previous orthodontic treatment.
The normal control group was recruited from the Institute for Postgraduate Dental Education, Jönköping, Sweden. These subjects had normal sagittal occlusion and no crossbite or other malocclusion traits, and were matched for age and dental age to the treated subjects.
The patients and their parents were given detailed oral and written information about the trial by 5 experienced general dental practitioners, who then treated the patients under the supervision of specialist orthodontists, according to a preset standard concept. The ethics committee of Lund University, Lund, Sweden, which follows the guidelines of the Declaration of Helsinki, approved the informed consent form and protocol (LU 399-00).
Study casts were made for the patients at baseline or pretreatment (T0), posttreatment (T1), and 3 years posttreatment (T2). For the control subjects with normal occlusion, 2 registrations were made: at T0 and T2 (at least 4 years after T0).
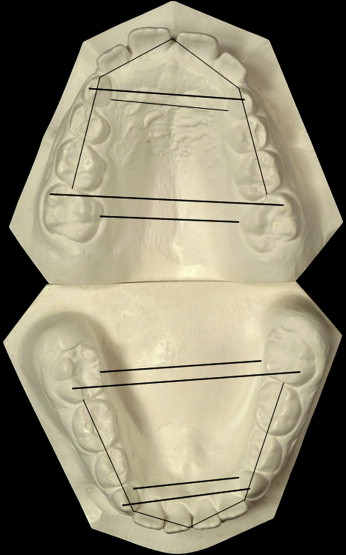
For the treated patients, the main outcome to be assessed was the success rate of crossbite correction. For both the treated and normal control subjects, the measurements included maxillary and mandibular intercanine and intermolar changes at the shortest linear distance at the gingival margins and the cusp tips of the teeth ( Fig 2 ). Overbite, overjet, midline deviation, and arch length in both jaws were registered. Midline deviation was defined as the discrepancy between the maxillary and mandibular midlines.
Intercanine and intermolar measurements were made to the nearest 0.1 mm, by using a digital sliding caliper (digital 6, 8M007906, Mauser, Winterthur, Switzerland). One orthodontist (S.P.) undertook all measurements. Overbite and overjet were measured to the nearest 0.5 mm with a stainless steel ruler. Assessment of transverse occlusion (crossbite correction) and all study cast measurements were blinded; ie, the examiner was unaware of the group to which the patient belonged. Furthermore, the T0, T1, and T2 casts were randomized for measurement.
The quad-helix appliance consisted of a standard stainless steel arch (MIA system, 3M Unitek, Monrovia, Calif) with stainless steel bands cemented onto the maxillary first molars with glass ionomer cement ( Fig 3 ). The quad-helix was activated 10 mm before placement and then, when necessary, reactivated every 6 weeks until a normal transverse relationship was achieved: no overcorrection. To prevent or compensate for buccal tipping, the appliance was adjusted for buccal root torque. The treatment result was retained for 6 months.

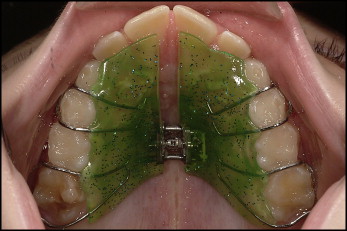
The expansion plate was made of acrylic, with an expansion screw and stainless steel clasps on the first deciduous and permanent molars ( Fig 4 ). The patient activated the screw 0.2 mm once a week until a normal transverse relationship was achieved: no overcorrection. The patient was instructed clearly to wear the plate night and day, except for meals and toothbrushing. The treatment result was retained for 6 months.
Twenty randomly selected study casts were measured on 2 occasions. Paired t tests disclosed no significant mean differences between the 2 series of records. The error of the method did not exceed 0.2 mm for any study variable.
Statistical analysis
The sample size for each group had previously been calculated and was based on a significance level of α = 0.05 and a power (1-β) of 90%, to detect a mean intergroup difference in expansion of 2 mm (±1.5 mm). The sample size calculation showed that each group needed a minimum of 12 subjects. To increase the power further and to compensate for possible attrition, it was decided to add 10 more subjects to the follow-up study.
The data were statistically analyzed by using SPSS software (version 16.0, SPSS, Chicago, Ill). The Fisher exact test was used to calculate the success rates of crossbite correction and midline deviation. For numeric variables, the arithmetic means and standard deviations were calculated. Analysis of variance (ANOVA) with the Tukey post-hoc test was used to compare changes within and between groups. Differences with probabilities of less than 5% ( P <0.05) were considered statistically significant.
Results
There were no significant differences at T0 between the treated groups with respect to age or crossbite side. Since no significant sex differences were found for any of the study variables, the data for the sexes were pooled for analysis.
The T0 measurements of the jaws are summarized in Table II . The crossbite subjects had significantly smaller values for all maxillary variables. With respect to the mandibular variables—overbite, overjet, and arch length—no intergroup differences were found, except that the arch lengths of quadrants 2 and 4 in the control group were greater than in the crossbite groups. The prevalences of midline deviation at T0 were 19 of 20 in the quad-helix group, 14 of 15 in the expansion-plate group, and 10 of 20 in the normal group.
| Quad-helix (A) n = 20 |
95% CI for mean |
Expansion plate (B) n = 15 |
95% CI for mean |
Normal group (C) n = 20 |
95% CI for mean |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline records | Mean | SD | Lower | Upper | Mean | SD | Lower | Upper | Mean | SD | Lower | Upper | Group difference |
| Maxilla | |||||||||||||
| Intermolar distance, gingival margin | 29.7 | 2.44 | 28.5 | 30.8 | 29.9 | 2.3 | 28.6 | 31.2 | 33.6 | 2.72 | 32.3 | 34.9 | C>A,B ‡ |
| Intermolar distance, mesiobuccal cusp tips | 47.1 | 2.62 | 45.9 | 48.3 | 46.7 | 2.39 | 45.3 | 48 | 50.6 | 2.49 | 49.4 | 51.7 | C>A,B † |
| Intercanine distance, gingival margin | 22.8 | 1.29 | 22.2 | 23.4 | 22.8 | 1.78 | 21.8 | 23.7 | 25 | 2.35 | 23.9 | 26.1 | C>A † ; C>B † |
| Intercanine distance, buccal cusp tips | 29.4 | 1.82 | 28.5 | 30.2 | 30.1 | 2.13 | 29 | 31.3 | 32.5 | 2.31 | 31.4 | 33.6 | C>A ‡ ; C>B † |
| Mandible | |||||||||||||
| Intermolar distance, gingival margin | 33.4 | 2.39 | 32.3 | 34.5 | 33.2 | 2.49 | 31.8 | 34.6 | 33.1 | 1.54 | 32.4 | 33.8 | NS |
| Intermolar distance, mesiobuccal cusp tips | 45.6 | 2.9 | 44.2 | 46.9 | 45.2 | 2.88 | 43.7 | 46.8 | 44.9 | 2.15 | 43.9 | 45.9 | NS |
| Intercanine distance, gingival margin | 20.7 | 1.6 | 20 | 21.5 | 20.7 | 1.38 | 19.8 | 21.5 | 21 | 1.5 | 20.3 | 21.7 | NS |
| Intercanine distance, buccal cusp tips | 26 | 2 | 25.1 | 27 | 26.3 | 1.3 | 25.5 | 27.1 | 26.9 | 1.5 | 26.1 | 27.6 | NS |
| Overjet | 2.9 | 1.33 | 2.3 | 3.5 | 3.2 | 1.5 | 2.3 | 4 | 4 | 2.4 | 2.9 | 5.1 | NS |
| Overbite | 2.4 | 1.31 | 1.8 | 3 | 2.1 | 1 | 1.5 | 2.6 | 2.3 | 2.1 | 1.4 | 3.4 | NS |
| Arch length quadrant 1 | 36.9 | 1.95 | 36 | 37.8 | 37 | 1.25 | 36.4 | 37.7 | 38 | 2.66 | 36.8 | 39.3 | NS |
| Arch length quadrant 2 | 37.3 | 2.1 | 36.3 | 38.3 | 36.7 | 1.16 | 36 | 37.3 | 38.6 | 1.62 | 37.8 | 39.3 | C>B † |
| Arch length quadrant 3 | 35.2 | 1.49 | 34.5 | 35.9 | 35 | 1.26 | 34.3 | 35.7 | 35.3 | 1.64 | 34.5 | 36.1 | NS |
| Arch length quadrant 4 | 34.3 | 1.94 | 33.5 | 35.3 | 35.3 | 1.24 | 34.6 | 35.9 | 35.6 | 1.36 | 35 | 36.3 | C>A∗ |
The changes during the treatment period (T0-T1) are summarized in Table III . The maxillary intermolar and intercanine distances increased significantly in both treatment groups. Mandibular intermolar expansion was significantly greater in the expansion-plate group than in the quad-helix group. There were no intergroup differences with respect to overbite or overjet. The arch length in quadrant 3 was greater in the expansion-plate group than in the quad-helix group. After treatment, a correct midline was achieved in more than half the crossbite patients, but there was no significant inter-group difference.
| Quad=helix (A) n = 20 |
95% CI for mean |
Expansion plate (B) n = 15 |
95% CI for mean |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Difference records T1-T0 | Mean | SD | Lower | Upper | Mean | SD | Lower | Upper | Group difference |
| Maxilla | |||||||||
| Intermolar distance, gingival margin | 3.7 ‡ | 1.58 | 2.9 | 4.4 | 3.2 ‡ | 1.24 | 2.5 | 3.9 | NS |
| Intermolar distance, mesiobuccal cusp tips | 4.1 ‡ | 1.45 | 3.5 | 4.8 | 3.8 ‡ | 1.62 | 2.9 | 4.7 | NS |
| Intercanine distance, gingival margin | 1.5 † | 1.64 | 0.7 | 2.3 | 2.4 ‡ | 1.44 | 1.5 | 3.3 | NS |
| Intercanine distance, buccal cusp tips | 2.7 ‡ | 1.57 | 1.9 | 3.4 | 2.6 ‡ | 1.58 | 1.7 | 3.6 | NS |
| Mandible | |||||||||
| Intermolar distance, gingival margin | −0.4 | 0.82 | −0.7 | 0 | 0.4∗ | 0.67 | 0 | 0.8 | B>A † |
| Intermolar distance, mesiobuccal cusp tips | −0.1 | 1.4 | −0.8 | 0.5 | 1.2 ‡ | 0.7 | 0.8 | 1.5 | B>A † |
| Intercanine distance, gingival margin | 0.2 | 1.05 | −0.3 | 0.8 | 0.6 | 1.63 | −0.6 | 1.7 | NS |
| Intercanine distance, buccal cusp tips | −0.5 | 1.21 | −1.1 | 0.1 | 0.5 | 1.42 | −0.5 | 1.5 | NS |
| Overjet | −0.1 | 0.83 | −0.5 | 0.3 | 0 | 1.32 | −1.2 | 0.3 | NS |
| Overbite | 0.2 | 0.92 | −0.3 | 0.6 | 0.6 | 1.03 | 0 | 1.1 | NS |
| Arch length quadrant 1 | 0.5 | 1.05 | 0 | 1 | 0.6 | 1.32 | −0.1 | 1.3 | NS |
| Arch length quadrant 2 | 0 | 1.91 | −0.9 | 0.9 | 1 † | 0.87 | 0.5 | 1.5 | NS |
| Arch length quadrant 3 | −0.7∗ | 1.24 | −0.1 | −0.1 | 0.4 | 0.93 | −0.1 | 0.9 | B>A † |
| Arch length quadrant 4 | −0.3 | 1.76 | −1.1 | 0.5 | −0.2 | 0.91 | −0.7 | 0.3 | NS |
At 3 years posttreatment, all 15 patients in the expansion-plate group and 19 of the 20 patients in the quad-helix group had normal transverse relationships; ie, the treatment outcome was longitudinally stable. However, during the posttreatment period, significant decreases in maxillary and mandibular transverse dimensions occurred in the treatment groups. There were no significant intergroup differences, except for mandibular intermolar distance at the gingival margin, which decreased more in the expansion-plate group ( Table IV ). The corrected midlines in the treatment groups relapsed in some patients, but there were also a few spontaneous corrections. Moreover, during the observation period, both spontaneous midline corrections and deviations occurred in the control group.
| Quad-helix (A) n = 20 |
95% CI for mean |
Expansion plate (B) n = 15 |
95% CI for mean |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Difference records T2-T1 | Mean | SD | Lower | Upper | Mean | SD | Lower | Upper | Group difference |
| Maxilla | |||||||||
| Intermolar distance, gingival margin | −0.8∗ | 1.48 | −1.5 | −1.5 | −0.6 | 1.14 | −1.2 | 0 | NS |
| Intermolar distance, mesiobuccal cusp tips | −0.8 | 1.7 | −1.5 | 0 | −0.4 | 1.33 | −1.1 | 0.4 | NS |
| Intercanine distance, gingival margin | −1.2 ‡ | 1.19 | −1.8 | −0.6 | −1.4∗ | 1.54 | −2.4 | −0.3 | NS |
| Intercanine distance, buccal cusp tips | 0.4 | 1.67 | −0.4 | 1.3 | 0.2 | 1.09 | −0.5 | 0.9 | NS |
| Mandible | |||||||||
| Intermolar distance, gingival margin | −0.2 | 0.92 | −0.7 | 0.2 | −1 † | 1.15 | −1.6 | −0.4 | B>A∗ |
| Intermolar distance, mesiobuccal cusp tips | −0.5 | 1.2 | −1.04 | 0 | −1.3 † | 1.16 | −1.9 | −0.6 | NS |
| Intercanine distance, gingival margin | −1 † | 1.1 | −1.6 | −0.4 | −1.8∗ | 1.4 | −2.8 | −0.9 | NS |
| Intercanine distance, buccal cusp tips | 0.1 | 1.29 | −0.6 | 0.8 | −0.7 | 1.35 | −1.6 | 0.2 | NS |
| Overjet | 0.4 | 1 | 0 | 0.9 | 0.3 | 0.7 | −0.1 | 0.7 | NS |
| Overbite | 0.5 | 1.18 | 0 | 1.1 | 0.5 | 1.1 | −0.1 | 1.1 | NS |
| Arch length quadrant 1 | −0.6 | 1.19 | −1.2 | −0.1 | −0.8 | 2.15 | −2 | 0.4 | NS |
| Arch length quadrant 2 | −0.1 | 1.28 | −0.7 | 0.5 | −0.3 | 1.04 | −0.9 | 0.3 | NS |
| Arch length quadrant 3 | −1.2 | 1.62 | −1.9 | −0.4 | −1.7 | 1.42 | −2.5 | −1 | NS |
| Arch length quadrant 4 | −1.2 | 1.32 | −1.8 | −0.6 | −1.5 | 1.13 | −2.1 | −0.9 | NS |
The overall changes during the 4-year study period (T0-T2) are shown in Table V . Significant increases in maxillary transverse distances were found in all groups ( P <0.01), except for intercanine distance at the gingival margin. There was no significant intergroup difference in expansion, except for maxillary intermolar cusp tip distance, which was greater in the treatment groups than in the control group. In the mandible, there were small, albeit significant, differences in the groups, but no intergroup differences except for intermolar distance at the gingival margin, which was greater in the control group than in the treated groups.
| Quad-helix (A) n = 20 |
95% CI for mean |
Expansion plate (B) n = 15 |
95% CI for mean |
Normal group n = 20 |
95% CI for mean |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Difference records T2-T0 | Mean | SD | Lower | Upper | Mean | SD | Lower | Upper | Mean | SD | Lower | Upper | Group difference |
| Maxilla | |||||||||||||
| Intermolar distance, gingival margin | 2.8 ‡ | 1.71 | 2 | 3.6 | 2.6 ‡ | 1.19 | 1.9 | 3.3 | 2 ‡ | 1.66 | 1.2 | 2.8 | NS |
| Intermolar distance, mesiobuccal cusp tips | 3.4 ‡ | 1.38 | 2.7 | 4 | 3.5 ‡ | 1.19 | 2.8 | 4.1 | 1.9 ‡ | 1.58 | 1.2 | 2.6 | A,B>C † |
| Intercanine distance, gingival margin | 0.2 | 1.88 | −0.7 | 1.1 | 0.6 | 2.25 | −0.8 | 2.1 | −0.2 | 2.12 | −1.2 | 0.8 | NS |
| Intercanine distance, buccal cusp tips | 3.2 ‡ | 2.28 | 2.1 | 4.3 | 2.5 ‡ | 1.68 | 1.5 | 3.5 | 1.6† | 2.38 | 0.5 | 2.7 | NS |
| Mandible | |||||||||||||
| Intermolar distance, gingival margin | −0.6∗ | 1 | −1.1 | −0.1 | −0.6 | 1.2 | −1.2 | 0 | 0.5∗ | 1.03 | 0 | 1 | C>A,B † |
| Intermolar distance, mesiobuccal cusp tips | −0.6 | 1.33 | −1.2 | 0 | −0.1 | 1.2 | −0.8 | 0.6 | 0 | 1.32 | −0.6 | 0.7 | NS |
| Intercanine distance, gingival margin | −1 † | 1.16 | −1.6 | −0.4 | −1.3 † | 1.19 | −2 | −0.5 | −1.6 ‡ | 1.16 | −2.1 | −1.1 | NS |
| Intercanine distance, buccal cusp tips | −0.7 | 1.6 | −1.5 | 0.2 | −0.4 | 1.12 | −1.1 | 0.2 | −0.4 | 1.64 | −1.1 | 0.4 | NS |
| Overjet | 0.4 | 1.41 | −0.3 | 1 | −0.2 | 1.27 | −0.9 | 0.5 | −0.6 | 2.16 | −1.6 | 0.5 | NS |
| Overbite | 0.7 | 1.38 | 0 | 1.3 | 1.1 | 1.16 | 0.4 | 1.7 | 0.8 | 1.34 | 0.1 | 1.4 | NS |
| Arch length quadrant 1 | −0.2 | 1.7 | −1 | 0.6 | −0.2 | 1.5 | −1.1 | 0.6 | 0.7 | 2.29 | −0.3 | 1.8 | NS |
| Arch length quadrant 2 | 0 | 2.03 | −1 | 0.9 | 0.7 | 1.42 | −0.1 | 1.5 | −0.1 | 1.68 | −0.9 | 0.7 | NS |
| Arch length quadrant 3 | −1.9 | 1.62 | −2.6 | −1.1 | −1.4 | 1.5 | −2.2 | −0.5 | −1.4 | 1.49 | −2.1 | −0.7 | NS |
| Arch length quadrant 4 | −1.5 | 1.89 | −2.4 | −0.6 | −1.7 | 1.13 | −2.3 | −1.1 | −1.3 | 1.57 | −2 | −0.5 | NS |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


