A dentigerous cyst is the most common developmental odontogenic cyst. It is a benign and asymptomatic intraosseous lesion that affects the bones of the maxillofacial complex, interfering with tooth eruption. This article reports the spontaneous eruption of a canine after marsupialization of an infected dentigerous cyst and extraction of the deciduous teeth. A radiograph showed a large cyst with a radiolucent area involving the mandibular left deciduous canine and first molar, and the permanent canine and first premolar. Although enucleation is the treatment of choice, marsupialization is the best option for large cysts involving an unerupted permanent tooth, as in this case. The patient was followed for 1 year, and eruption of the permanent canine and first premolar and gradual reduction of the radiolucent area were observed.
A dentigerous cyst is the most prevalent type of developmental odontogenic cyst. Its origin is in the tooth follicle of an unerupted tooth crown, generally the mandibular third molar, which is attached to the cyst through the cementoenamel junction. Its pathogenesis is unknown, but it can be explained by the accumulation of liquid between the remnants of the reduced enamel epithelium of the tooth-forming organ and the unerupted tooth crown after its complete development.
It is more frequent in the second and third decades of life, with a male predilection, and the mandible is the most affected region. These cysts can cause cortical bone expansion and consequently facial asymmetry, although usually there are no symptoms. Dislocation of the teeth near the cyst and root resorption are also observed in some patients.
The radiographic image of a dentigerous cyst shows a unilocular radiolucent area with well-defined sclerotic margins. However, trabecular bone can appear on the radiographic images, creating a false impression of a multilocular lesion, and, once infected, the cyst can show diffuse margins.
Enucleation and marsupialization are the best options to treat a dentigerous cyst. The first is the process in which the cyst is completely removed without rupture; this is generally indicated for small cysts. For large lesions, this procedure can cause fracture of the mandible, tooth devitalization, or removal of impacted teeth associated with the lesions that do not need to be removed. Marsupialization consists of a surgical cavity on the wall of the cyst, emptying its content and maintaining the continuity between the cyst and the oral cavity, maxillary sinus, or nasal cavity, but it is not indicated for infected lesions. This technique is indicated for large cysts, unerupted teeth associated with cysts in pediatric patients, or in patients with systemic diseases, generally the elderly. It permits decompression of the cyst, reducing the extent of the bone defect.
The treatment of impacted teeth is a challenge to orthodontists, and the treatment of choice is surgical exposure of the tooth and consequent orthodontic traction, which generally causes a cyst cavity reduction and preserves the unerupted tooth. Spontaneous eruption, without orthodontic intervention, can occur after the extraction of deciduous teeth and cyst marsupialization. It is generally known that there is a close relationship between the ability of a tooth to erupt and the level of dental root formation. A permanent tooth breaks through the alveolar bone and erupts when approximately two thirds of the root has formed and then erupts into the oral cavity at approximately three fourths to complete root formation with a wide-open apex.
We present a case report of a patient with an unerupted mandibular left permanent canine and first premolar associated with an infected dentigerous cyst that was treated with marsupialization therapy. We performed the marsupialization technique, considering the possibility of physiologic eruption of permanent teeth associated with the cyst, followed by orthodontic support.
Case report
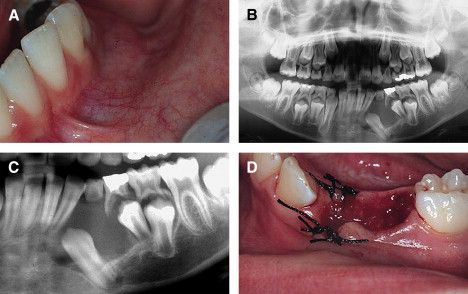
A healthy 9-year-old boy was referred by his general dentist who suspected a dentigerous cyst associated with a mandibular left deciduous canine and intraosseous premolar. There had been evidence of recent fever episodes and intraoral purulent discharge related to the deciduous canine and first molar; the patient had been treated with antibiotics. Clinical examinations showed extra and intraoral hardened and painless swelling and mobility of the involved teeth ( Fig 1 , A ). The panoramic radiograph showed a large, well-defined radiolucent lesion measuring 3.0 × 4.0 cm associated with the deciduous canine and first premolar, changing the eruption angulation of the permanent canine and premolar by about 15 mm ( Fig 1 , B and C ).
The objectives of this treatment were to reduce the size of lesion with the marsupialization technique, considereded less aggressive, and to follow up orthodontically the eruption of the permanent canine and first premolar, establishing a favorable oclusion, with good functional and esthetic results.
Two treatment alternatives were considered, enucleation and marsupialization, which could be used after extraction of the involved deciduous teeth. The first alternative, enucleation, is usually the technique of choice for small lesions because, in larger lesions, enucleation can cause extensive damage to the adjacent teeth and to the teeth involved in the lesion. Marsupialization is the treatment option for extensive lesions, especially in pediatric patients, as in this report.
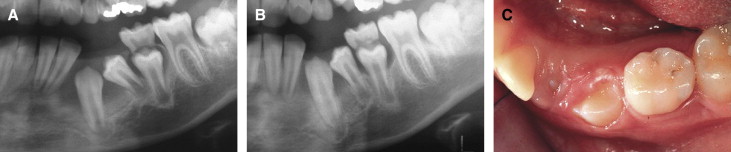
A local incision was made, showing a small amount of cystic liquid, confirmed by histopathologic examination. The treatment performed was marsupialization of the cyst and extraction of the deciduous canine and first molar ( Fig 1 , D ). The surgical stitches were removed a week after the procedure. Approximately 3 months later, the cystic lesion diminished, and eruption of the permanent canine and first premolar in normal positions was observed ( Fig 2 ).
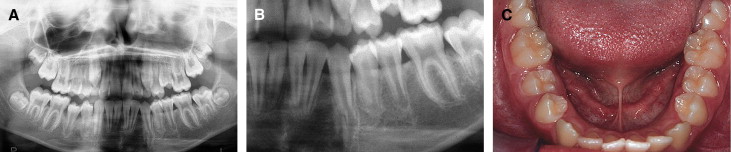
After 1 year, the radiograph and clinical features showed reduction of the swollen area, spontaneous eruption of the mandibular left canine and first premolar, and aspects of normality after marsupialization of the dentigerous cyst. After this, any orthodontic biomechanics treatment could be used ( Fig 3 ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


