Introduction
The purposes of this study were to evaluate whether unaltered elastomeric chain can continue to move teeth for 16 weeks and to relate it to the amount of force remaining for the same batch of elastomeric chains.
Methods
The in-vivo portion of the study had a sample of 30 paired extraction space sites from 22 subjects who were measured for closure of the space every 28 days. The altered side elastomeric chain served as the control and was replaced at 28-day intervals whereas the experimental side remained unaltered. In the in-vitro portion of the study, 100 each of 2-unit and 3-unit segments of the same batch of elastomeric chains were placed in a water bath, and the force was measured for 20 of each segment length at the 28-day measurement points.
Results
Statistically significant amounts of space closure occurred at both the altered and unaltered sites at all measurement time points. The mean space closure at the altered sites was minimally greater than that observed at the paired unaltered sites. The mean differences of space closure between the altered and unaltered sites ranged from a minimum of –0.05 mm at 4 weeks to a maximum of –0.14 mm at 8 weeks. The elastomeric chain force degraded rapidly by 4 weeks but continued a gradual diminution of force to 86 g at 16 weeks.
Conclusions
Unaltered elastomeric chain continued to move teeth into extraction spaces for 16 weeks in this sample from both statistically and clinically significant standpoints. There were minimal and statistically insignificant differences in the mean space closure measurements between the paired altered and unaltered sites. The elastomeric chain force at 16 weeks was less than 100 g, yet at the same time point, teeth continued to move clinically.
Highlights
- •
Elastomeric chains can continue to move teeth for a minimum of 16 weeks.
- •
Elastomeric chain measured in vitro demonstrated diminishing force to a mean of 86 g at 16 weeks.
- •
Use of a practice-based network of clinicians is a promising approach for clinical research.
Orthodontists have always had a need to close spaces created by extraction of permanent teeth. Consequently, numerous mechanisms have been used to close these extraction spaces. Some commonly used examples are closing loops, coil springs, elastics, and elastomeric chains. In the mid 1960s, Roland Anderson and Paul Klein had the idea for using an elastic material for archwire ties. They developed an elastomeric material, patented the process, and formed a company (Modcom) to produce AlastiK products. The Unitek Corporation purchased the products and began marketing to the orthodontic community in 1968.
Research was first published on elastomeric chain by Andreasen and Bishara in 1970. Other investigators have provided information to describe the benefits of elastomeric chains such as low cost, ease of use, and reduced need for patient compliance. However, there are the disadvantages of increased entrapment of biofilm and the degradation of elastic force through time as determined by predominantly in-vitro studies.
Elastomeric chains are synthetic elastomers. They are primarily made from polyurethane, which can be either thermoplastic or thermoset. Thermoplastic polyurethanes are moldable at high temperatures and can be made from plastic. It has been shown that these chains experience more force decay at 28 days in vitro and require less prestretching than do thermoset chains.
Thermoset materials are cured irreversibly during manufacturing and have been shown to decay less in vitro. Elastomeric chains produced by different manufacturers generate various initial force levels when stretched the same amount. Most elastomeric chains experience force decay of 50% to 70% in the first 24 hours, followed by a more stable phase of 10% to 20% force decay in the first 4 weeks. There is limited information on the rate of decay past this 4-week point. The force decay loss is due to permanent deformation of the elastomer when polymer molecules irreversibly slide past each other. Few in-vivo studies have been done to study the potential decay of elastomeric chain. Since there is a loss of force over time, clinicians typically replace the chain in a patient’s mouth every 4 to 6 weeks. However, since the chains probably retain some level of force past 4 weeks, it is unknown whether the force remaining is sufficient to move teeth in a clinical environment. It has been shown that in a simulated oral environment with a basic pH (7.26), force degradation occurs more rapidly than in an acidic pH (4.95) environment or in air.
Anecdotally, when there has been an inadvertent nonreplacement of elastomeric chain, a continued closure of space over a much longer than anticipated time frame can often be observed. The clinical question then arises: “why would the space continue to close with an elastomeric chain that should have worn out?” In this study, we tested the primary hypothesis: unaltered elastomeric chains continue to produce extraction space closure over a 16-week period in a patient’s mouth. In addition, to relate the space closure to the predicted force degradation of elastomeric chain material, in the in-vitro component of the study, we tested the force degradation for 16 weeks of the same batch of elastomeric chain that was used in the clinical component.
Material and methods
For the in-vitro component, 2 wood jigs were constructed with 10 pairs of steel finishing nails placed 10 mm apart on 1 jig and 18 mm apart on the other. One hundred each of 2-unit and 3-unit elastomeric chain (AlastiK Gray Spool Chain C-1 Medium Force, Lot No. GG9WJ; 3M Unitek, Monrovia, Calif) segments were stretched twice their resting length on the 10-mm and 18-mm pegs, respectively. The jigs were submerged in a distilled water bath at 37°C ( Fig 1 ) to partially simulate the oral environment. A 600-g spring gauge (Pesola, Schindellegi, Switzerland) was used to measure 20 samples for the initial force of the 2-unit and 3-unit segments at twice the resting length. Twenty samples of each segment length were removed from the jigs at every 28-day time point (4, 8, 12, and 16 weeks), and the force was measured at the respective 10-mm and 18-mm stretchings. The distilled water was replaced at each measurement time point.

For the in-vivo component, a practice-based clinical research network of 23 volunteer orthodontic clinicians was approached to participate in the research and provide patients for the study. Sixteen agreed to the research protocol. The clinicians were asked to select as many extraction patients as possible from their practices who would meet the study’s selection criteria. Appropriate consent for the research project was obtained from Vanderbilt University’s institutional review board.
A split-mouth research design was used in each arch, with 1 extraction side serving as the control site (altered elastomeric chain) and the contralateral extraction side serving as the experimental site (unaltered elastomeric chain), thus creating paired sites in each arch. A precise research protocol was issued to each participating orthodontist. It delineated the case selection criteria: adolescent patient, less than 16 years of age, with bilateral premolar extractions in the maxillary or the mandibular arch, or in both arches. Each patient’s parent was made aware of the research project and its implications for treatment. All parents of participating subjects signed an informed agreement of participation.
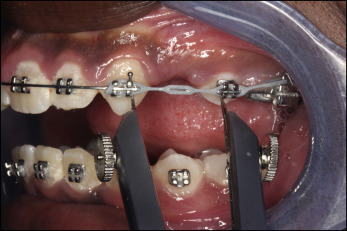
After leveling and alignment of the patient’s arches, the clinician decided when to commence space closure. The requirements for space closure involved sliding mechanics with no auxiliaries and either segmental extraction space closure (canine retraction or reciprocal molar to premolar) or total arch en-masse extraction space closure. For en-masse space closure, the teeth anterior to the extraction space were stabilized as a section with either wire ligature or elastomeric chain. This enabled the extraction sites to be handled independently of the anterior segment of the arches. The same thermoplastic elastomeric chain production batch (AlastiK Gray Spool Chain C-1 Medium Force, Lot No. GG9WJ) was provided to the participating clinicians and used for all subjects. Sectional chains were placed on both sides of an arch from the most distal tooth with a bracket to the tooth on the mesial side of the extraction space (from a mandibular first molar to a mandibular first premolar in case of a second premolar extraction). The clinician selected the side that served as the control (altered elastomeric chain) with the segmental elastomeric chain replaced every 28 ± 5 days. The contralateral side served as the experimental side (unaltered elastomeric chain), and the elastomeric chain was not replaced. Clinicians measured the closure of the each extraction space using the same intraoral reference points (between brackets on the teeth or tooth surfaces) at every time measurement point. The intraoral measurement was made using one of the following: an electronic caliper, a Boley gauge with vernier scale, or a sharp pointed mechanical divider and ruler ( Fig 2 ). Measurements to a tenth of a millimeter were placed on a recording data sheet provided for each participating patient. A 16-week experimental time was selected for the clinically pragmatic reason that orthodontists and their patients would likely not risk the lack of extraction space closure for a longer period of time. There was a 6-month experimental time window in which to accomplish the 16 weeks of space closure per subject. In other words, each clinician could begin a selected extraction patient at the beginning of the first month and have 2 months to continue to select patients for the study. The recording data sheets were collected from the participating clinicians at the end of the experimental time period. Those data were recorded, and appropriate statistical manipulations were performed and presented in the results.
A portion of the experimental protocol pertained to the criteria for disqualification of a subject during the experimental time period that would end the subject’s involvement in the project. Those reasons were as follows: (1) if a subject appeared at his or her appointment with either the unaltered site or the altered site elastomeric chain broken or missing; (2) if at the unaltered site the elastomeric chain was inadvertently removed during the experimental time or the extraction space became closed; and (3) if the time between monthly measurements exceeded 33 days. After disqualification of a subject, all previous measurements would be acceptable data.
Results
Of the 16 clinicians who consented to participate in this study, only 8 were able to contribute patients to the study’s sample. The sample comprised 22 extraction patients using a split-mouth design for each arch. There were a total of 31 paired sites composed of a control side (altered site) where the elastomeric chain was replaced every 28 days and an experimental side (unaltered site) where the original elastomeric chain remained in place. One paired site did not have the first 4-week measurement because of resignation of the subject. Thus, the subsequent analysis was based on 30 paired extraction sites.
The first evaluation used the actual space closure reduction between 2 consecutive measurement time points for each extraction space. A positive value would indicate a reduction in space. For each follow-up measurement, we conducted a 2-sided 1-sample t test to assess whether the space closure was significantly different from zero. Table I presents the summary statistics and the t test results for all the sites measured at each time point. Not surprisingly, we observed statistically significant amounts of space closure for the altered sites with mean reductions of 1.62, 1.05, 1.03, and 0.97 mm at the measurement time points of 4, 8, 12, and 16 weeks, respectively. The space closure values for the unaltered sites were also significantly different from zero at all follow-up times, with means of 1.57, 0.91, 0.98, and 0.85 mm for the respective measurement points. The sample size became smaller at each measurement point. At week 8, 3 subjects dropped out, reducing the sample to 27 paired sites, and 1 altered site space became closed. By the end of the study at week 16, 12 (40%) unaltered sites were completely closed (3 closed at 8 weeks, 4 closed at 12 weeks, and 5 closed at 16 weeks). For the altered sites, there was space closure at week 16 for 13 (43%) sites (1 closed at 4 weeks, 1 closed at 8 weeks, 6 closed at 12 weeks, and 5 closed at 16 weeks).
| Time point (wk) | Site | n | Mean (mm) | SD | Minimum | Maximum | 95% CI | Two-sided 1-sample t test | |
|---|---|---|---|---|---|---|---|---|---|
| t | P | ||||||||
| 4 | Unaltered | 30 | 1.57 | 0.81 | 0.5 | 4.3 | 1.27-1.87 | t (29) = 10.65 | >0.001 |
| Altered | 30 | 1.62 | 0.92 | 0.3 | 3.7 | 1.27-1.96 | t (29) = 9.61 | >0.001 | |
| 8 | Unaltered | 27 | 0.91 | 0.63 | 0.0 | 2.1 | 0.66-1.16 | t (26) = 7.48 | >0.001 |
| Altered | 26 | 1.05 | 0.56 | 0.3 | 2.2 | 0.83-1.28 | t (25) = 9.67 | >0.001 | |
| 12 | Unaltered | 23 | 0.98 | 0.64 | 0.0 | 2.6 | 0.71-1.26 | t (22) = 7.40 | >0.001 |
| Altered | 24 | 1.03 | 0.67 | 0.1 | 3.1 | 0.74-1.31 | t (23) = 7.46 | >0.001 | |
| 16 | Unaltered | 16 | 0.85 | 0.51 | 0.1 | 2.1 | 0.58-1.12 | t (15) = 6.68 | >0.001 |
| Altered | 15 | 0.97 | 0.53 | 0.2 | 2.2 | 0.67-1.27 | t (14) = 7.04 | >0.001 | |
The second evaluation was to determine to what extent the space closure was different between the unaltered and altered sites. We conducted a 2-sided paired t test to assess whether the difference in space closure between the altered and unaltered sites was statistically different from zero. The summary statistics appear in Table II . At week 4 after initial placement of chain at all sites, the mean reduction of the unaltered sites was smaller than that of the altered sites by 0.05 mm, which was 6% of the standard deviation for the differences. The 95% confidence interval (CI) at 4 weeks was −0.39 to 0.29; a confidence interval including 0 suggested that the difference between the unaltered and altered sites was statistically indistinguishable from zero. Similarly, at week 8, the reduction for the unaltered sites was smaller than that for the altered sites by 0.14 mm or 21% of the standard deviation; at week 12, the difference was 0.08 mm or 12% of the standard deviation, and at week 16, the difference was 0.07 mm or13% of the standard deviation. Overall average reduction for the unaltered sites was always smaller than the reduction for the altered sites at all measurement time points. However, the test results did not provide enough evidence to claim that the differences were statistically different from zero.
| Time point (wk) | n | Mean (mm) | SD | Minimum | Maximum | 95% CI | Two-sided paired t test | Two-sided paired t test (adjusting for correlated sites) | Sample size from power analysis | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| t | P | t | P | ||||||||
| 4 | 30 | −0.05 | 0.90 | −1.6 | 1.9 | −0.39 to 0.29 | t (29) = −0.29 | 0.772 | t (29) = −0.08 | 0.937 | 2748 |
| 8 | 26 | −0.14 | 0.68 | −1.6 | 1.5 | −0.42 to 0.13 | t (25) = −1.09 | 0.288 | t (25) = −1.07 | 0.293 | 175 |
| 12 | 23 | −0.08 | 0.66 | −1.7 | 1.3 | −0.37 to 0.21 | t (22) = −0.58 | 0.565 | t (22) = −0.42 | 0.680 | 531 |
| 16 | 15 | −0.07 | 0.59 | −0.8 | 1.0 | −0.40 to 0.25 | t (14) = −0.48 | 0.637 | t (14) = −0.19 | 0.849 | 508 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


