Introduction
The purpose of this study was to test whether girls are treated orthodontically for milder occlusal issues than are boys, thus accounting for the greater uptake of orthodontic services among girls compared with boys.
Methods
The dental aesthetic index (DAI) was used to score the severity of esthetic occlusal issues in 357 white adolescents. Half of the subjects were from private practices; the others were from a university specialty clinic.
Results
Average DAI scores were statistically significantly lower (milder) in girls than boys in both venues; this confirms the assumption that the actual uptake of services is greater in girls because of heightened concern for their esthetic occlusal issues. Average DAI scores predictably were higher in the teaching setting because of selection for more complex cases, but the sex difference was still evident statistically. There was no association between DAI score and age at the start of treatment among these adolescents. Spacing and incisor irregularity showed the greatest sex differences among the DAI variables, possibly because girls are more attuned to these esthetic issues.
Conclusions
These results complement studies that have recorded adolescents’ perceptions of orthodontic need. The actual uptake of orthodontic treatment is greater in girls because they (and their parents) seek treatment for milder occlusal issues.
Malocclusion is common in the United States and other developed countries, with most of the US population warranting orthodontic treatment. Misaligned teeth negatively impact a person’s life in areas such as mastication, speech, and, most importantly, appearance that involves psychological issues and subjective concerns of self-esteem. Orthodontic treatment can address a host of occlusal, periodontal, temporomandibular, and other issues, but the overwhelming reason that adolescents seek treatment is to improve their dental esthetics, notably the visible anterior teeth. Not all people who would benefit from orthodontic treatment actually seek treatment, but more than 30% of white, 11% of Hispanic, and 8% of African American youths reported having had some form of orthodontic treatment.
Epidemiologic studies show that males and females exhibit little difference in the overall prevalence of malocclusion. But, although malocclusions are not more prevalent or more severe in girls, girls receive a disproportionate amount of the orthodontic care in the United States and other countries. Girls not only are more likely to receive orthodontic treatment, but also are perceived to need orthodontic treatment more than boys by their parents and referring dentists. This sex difference is best documented in the United States, but it has also been quantified in other nations.
The purpose of this project was to help resolve these 2 seemingly disparate findings. Studies of orthodontic need and other epidemiologic studies have found few sex differences in the incidence or severity of malocclusions between boys and girls. Yet, orthodontic practices typically have appreciably more girls in treatment than boys. This suggests that there are social and cultural differences in the subjective perceived need for treatment, with a lower threshold for girls. The issue was whether the average female patient in the United States has a milder malocclusion than her male counterpart; this would confirm the hypothesis that perceptual factors, not severity of malocclusion per se, cause girls (and their caregivers) to seek treatment for milder esthetic issues.
Specifically, 2 questions were addressed: (1) whether girls have discernibly different esthetic occlusal scores than boys and (2) whether there are differences in esthetic scores between patients treated in a university-based teaching setting vs a private practice specialty venue.
Material and methods
We studied adolescent orthodontic patients (n = 357) who met these criteria:
- 1.
The patients received full-bonded comprehensive treatment with a starting age between 12 and 18 years, and in at least the early full permanent dentition with the permanent canines erupted because emergence of the canines often worsens the esthetic aspects of the occlusion. Also, it has been shown that adolescents are more concerned with their esthetics than are older persons.
- 2.
The patients were American whites with normal phenotypes (ie, no facial cleft, syndrome, or other condition that in itself predisposes for treatment). Intact dentitions were not a criterion for inclusion, since the number of missing teeth is measured as part of the severity of the malocclusion, so patients with extracted or congenitally absent teeth were included.
Half of the sample was collected from adolescents treated in the graduate orthodontic clinic at the University of Tennessee in Memphis. The other half was collected from private orthodontic specialty practices in the area. The intent was to test whether the graduate teaching setting, which selects for “good teaching cases” (ie, more complex malocclusions), removed any sex effect in the severity scores. Subjects were selected at random, but with the goal of obtaining equivalent sample sizes for the sexes.
The esthetic severity of each subject was assessed from the dental casts in maximum intercuspation by using the scoring system of Jenny and Cons, termed the dental aesthetic index (DAI). The method produces a summary score based on the weighted measurements of 10 variables, some of which have an ordinal scale, and others have a ratio scale. Greater DAI scores correspond to less esthetic occlusions. The 10 contributing measures of the score are listed below, and the values in parentheses are the weighting coefficients used to calculate the DAI.
- 1.
Number of missing teeth from among the incisors, canines, and premolars, with both arcades counted (5.76).
- 2.
Incisor crowding scored as 1 of 3 categories: 0, neither arch segment crowded; 1, 1 arch segment crowded; or 2, both arch segments crowded (1.15).
- 3.
Interdental incisor spacing, recorded as 0, no arch segment spaced; 1, 1 arch segment spaced; or 2, both arch segments spaced (1.31).
- 4.
Width of the midline diastema in millimeters (3.13). Because so many of these orthodontic patients had rotated maxillary central incisors and, thus, open contacts where a diastema would be, we measured only clear-cut subjects with an overt interdental gap and an obvious gingival space between the teeth. An open contact due to rotations or axial inclinations does not constitute a true diastema.
- 5.
Maxillary anterior tooth irregularity, recorded as the greatest maxillary discrepancy in millimeters between the anatomic contact points of the incisors and the canines (1.34).
- 6.
Mandibular anterior tooth irregularity measured analogously with the maxillary variable (0.75).
- 7.
Incisor overjet as the maximum horizontal distance measured in the more severe quadrant (1.62).
- 8.
Mandibular overjet was measured in place of variable 7 when there was an anterior crossbite or, synonymously, a negative overjet (3.68).
- 9.
Anterior open bite, the vertical millimetric distance measured when the incisor edges do not overlap (3.69).
- 10.
Buccal segment relationship was scored on a 3-grade ordinal scale: 0, Class I molar relationship; 1, one-half cusp discrepancy, either Class II or Class III; or 2, a full-cusp discrepancy (2.69).
After multiplying each measurement by its weighting coefficient, a constant of 13.36 was added to the sum to determine the DAI. The DAI originally was obtained from multiple linear regression, with 13.36 as the constant (Y intercept). The DAI can range from a minimum of 13.36 (the constant) up to some indefinite upper limit. Jenny and Cons offered a 4-grade classification of malocclusions using the DAI: 1, occlusion is normal or the malocclusion is minor (scores <25); 2, definite malocclusions, but treatment is elective (scores of 26-30); 3, severe malocclusions, with treatment highly desirable (scores of 31-35); and 4, very severe (handicapping) malocclusions, with treatment mandatory (scores >36). No index of malocclusion meets all needs, but the DAI has been adopted by the World Health Organization as a cross-cultural index.
The constituent data (the 10 variables forming the esthetic score) are a mix of ordinal and ratio scale variables, and each was evaluated statistically here by using appropriate statistics: chi-square analysis for the ordinal data and parametric tests ( t tests and analysis of variance [ANOVA]) for the continuous variables. Stepwise discriminant functions analysis was used to evaluate which variables contributed the most to the intergroup differences. Odds ratios were calculated as described by Agresti. Tests were 2-tailed, evaluated at the conventional level of alpha = 0.05. The crux of the study was to test whether girls have a lower score (milder, more esthetic malocclusion) than boys, and whether the more complex malocclusions expected in the university setting eliminated the sex differences. Thereafter, the pertinent question was which variables were driving the sex differences in esthetic scores in the groups.
Results
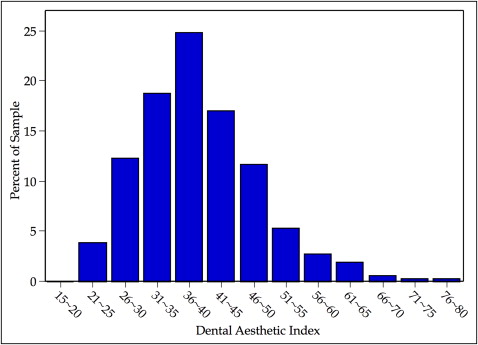
The distribution of the DAI scores for the total sample was unimodal and had approximately a Gaussian distribution ( Fig 1 ), but the lower portion of the distribution was truncated, since the milder cases did not warrant orthodontic intervention. The average score was 39.0 (median, 38.0). By using the 4-grade classification of Jenny and Cons, 4% of the patients were in the normal occlusion or minor need category, 12% exhibited definite malocclusions, 19% had severe malocclusions, and most (65%) had handicapping malocclusions, with treatment deemed obligatory.
A 2-way factorial ANOVA for the DAI disclosed both highly significant sex (F = 28.8; P <0.0001) and site (F = 29.5; P <0.0001) differences (university vs private setting), although the interaction term was not significant ( P = 0.523). In both settings, girls had significantly smaller (more esthetic, less severe) scores than boys. The sex difference between means was about 5 points ( Fig 2 ). That is, the sex difference in private practice (mean scores about 34 for girls and 40 for boys) was about the same as in the university setting (scores about 40 for girls and 44 for boys).
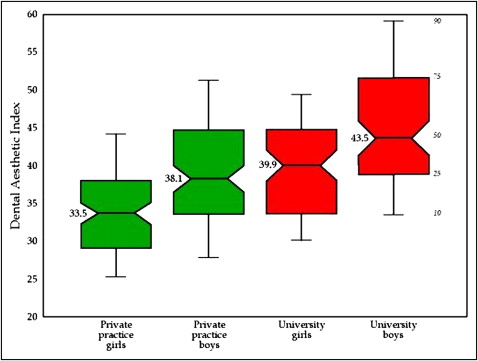
The highly significant site difference occurred because the average score in the private practice settings (DAI = 37) was smaller—milder malocclusions—than in the university setting (DAI = 42). This difference in distribution also is evident in Figure 2 , showing that the DAI scores for each sex shifted upward about 5 points in the teaching institution compared with the private practice setting.
The question arises why the highly significant sex and site differences occur—what occlusal features are responsible? Statistical tests were run on each of the 10 variables to determine the sources of significance ( Table ).
| Variable | University setting | Private practices | Sex difference | Site difference | ||||
|---|---|---|---|---|---|---|---|---|
| Boys (n = 75) | Girls (n = 75) | Boys (n = 100) | Girls (n = 107) | Test | P value | Test | P value | |
| Missing teeth | 7/75 | 5/75 | 9/100 | 7/107 | χ 2 = 0.58 | 0.7465 | χ 2 = 0.05 | 0.9737 |
| Incisor crowding | 59/75 | 55/75 | 66/100 | 77/107 | χ 2 = 1.33 | 0.5141 | χ 2 = 11.65 | 0.0030 |
| Incisor spacing | 31/75 | 26/75 | 53/100 | 31/107 | t = 11.90 | 0.0026 | t = 2.56 | 0.7286 |
| Diastema | x ¯ = 0.77 | x ¯ = 0.57 | x ¯ = 0.79 | x ¯ = 0.23 | t = 2.57 | 0.0104 | t = 1.05 | 0.2928 |
| SD = 1.81 | SD = 1.48 | SD = 1.71 | SD = 0.94 | |||||
| Maxillary irregularity | x ¯ = 4.19 | x ¯ = 4.11 | x ¯ = 3.11 | x ¯ = 2.76 | t = 1.37 | 0.1720 | t = 6.68 | <0.0001 |
| SD = 1.84 | SD = 1.68 | SD = 1.72 | SD = 1.50 | |||||
| Mandibular irregularity | x ¯ = 3.03 | x ¯ = 3.15 | x ¯ = 2.35 | x ¯ = 2.19 | t = 0.35 | 0.7236 | t = 5.10 | 0.0001 |
| SD = 1.51 | SD = 1.57 | SD = 1.30 | SD = 1.57 | |||||
| Maxillary overjet | x ¯ = 4.87 | x ¯ = 4.67 | x ¯ = 4.51 | x ¯ = 3.69 | t = 2.13 | 0.0339 | t = 2.42 | 0.0162 |
| SD = 3.18 | SD = 2.59 | SD = 2.47 | SD = 1.81 | |||||
| Mandibular overjet | x ¯ = 0.35 | x ¯ = 0.04 | x ¯ = 0.12 | x ¯ = 0.03 | t = 2.88 | 0.0081 | t = 1.71 | 0.0872 |
| SD = 1.20 | SD = 0.35 | SD = 0.54 | SD = 0.21 | |||||
| Anterior openbite | x ¯ = 0.37 | x ¯ = 0.16 | x ¯ = 0.30 | x ¯ = 0.12 | t = 2.05 | 0.0418 | t = 0.63 | 0.5272 |
| SD = 0.95 | SD = 0.61 | SD = 1.24 | SD = 0.53 | |||||
| Buccal segment relationship | 51/75 | 51/75 | 66/100 | 68/107 | χ 2 = 0.89 | 0.6418 | χ 2 = 0.84 | 0.6569 |
| DAI score | x ¯ = 39.55 | x ¯ = 35.88 | x ¯ = 35.36 | x ¯ = 30.14 | t = 5.15 | <0.0001 | t = 4.78 | <0.0001 |
| SD = 10.52 | SD = 7.93 | SD = 9.65 | SD = 7.34 | |||||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


