Introduction
In this study, we investigated the association between the severity of alveolar clefts in infants and the succeeding maxillofacial growth in patients affected by complete unilateral cleft lip and palate.
Methods
The subjects were 35 nonsyndromic patients affected by unilateral cleft lip and palate (n = 27) or bilateral cleft lip and palate (n = 8). Plaster models and lateral cephalograms taken at 6 years of age were analyzed and compared with the Japanese norms. In the unilateral cleft lip and palate patients, the relationship between the width of the alveolar cleft before palatoplasty and the skeletal characteristics was also explored.
Results
Significant deficiencies of the posterior maxilla and steep palatal planes were noted in both the unilateral and bilateral cleft lip and palate patients. However, they were not clearly observed in the unilateral cleft lip and palate patients born with a small alveolar cleft and were correlated with the severity of alveolar cleft in infancy. Neither cleft type nor the severity of the alveolar cleft was implicated in the maxillary arch form in childhood, but the growth of the alveolar height on the cleft side was less in the unilateral cleft lip and palate patients born with a large alveolar cleft.
Conclusions
The severity of the alveolar cleft before palatoplasty affects the succeeding vertical maxillofacial growth in patients affected by unilateral cleft lip and palate; this suggests the necessity of a different diagnosis and treatment in unilateral cleft lip and palate patients according to the severity of the alveolar cleft in infancy.
Patients affected by unilateral cleft lip and palate (UCLP) show characteristic patterns of maxillofacial growth. Typically, maxillary forward and downward growth is restricted, and patients have less convexity. On the other hand, symptoms of maxillary deficiency have much variation, and each patient shows individual differences. However, previous studies of craniofacial growth in UCLP patients have not described this variation. It might be a useful contribution for orthopedic treatment if the growth pattern of UCLP patients is predictable.
We have reported that the severity of the alveolar cleft significantly affected the prognosis of infant orthopedics in UCLP patients and influenced the difference of alveolar height between the affected and unaffected sides. We also noted that the severity of the alveolar cleft is an important key to predict maxillofacial growth in UCLP patients.
Several reports have indicated the relationship between the width of the cleft in newborn infants and craniofacial morphology in the children born with UCLP. Suzuki et al reported that the width of the cleft palate was associated with the lateral displacement of the nasomaxillary complex and the growth dysplasia of upper anterior facial height in UCLP patients at 4 years old. The width of the alveolar cleft at birth and the skeletal characteristics in UCLP patients at 5 years old were also correlated, but the authors studied only the anteroposterior jaw relationships. Few studies have extensively evaluated the relevance of the severity of the alveolar cleft and craniofacial growth in UCLP patients.
Therefore, we hypothesized that the severity of the alveolar cleft in UCLP patients might affect their maxillofacial growth in childhood. We investigated the association between the severity of the alveolar cleft before palatoplasty and the characteristics of maxillofacial morphology at 6 years of age in patients affected by complete UCLP with a 3-dimensional model evaluation and a cephalometric analysis, and compared them with patients affected by bilateral cleft lip and palate (BCLP) and the Japanese norms.
Material and methods
Twenty-seven nonsyndromic patients affected by complete UCLP and 8 patients affected by BCLP who consulted the outpatient clinic of the Department of Orthodontics and Dentofacial Orthopedics at Tokushima University Hospital in Japan from 1990 to 2005 served as our subjects. All patients had cheiloplasty with a triangular flap method approximately 3 months after birth and 1-stage palatoplasty with the push-back method at the mean age of 13 months by 2 senior surgeons of the Department of Reconstructive Plastic Surgery at Tokushima University Hospital. All patients also received infant orthopedic treatment with a palatal device for molding and positioning the alveolar segments (Hotz plate) as described by Hotz and Gnoinski from immediately after the cheiloplasty to just before the palatoplasty. The infant orthopedic treatment was part of the standard protocol in our department.
Records of the UCLP subjects (14 boys, 13 girls; mean age, 5.7 years; SD, 1.1 years) were compared with those of the BCLP subjects (6 boys, 2 girls; mean age, 5.8 years; SD, 1.1 years). The UCLP subjects were divided into 2 groups according to the width of the alveolar cleft immediately after the cheiloplasty (T1). The UCLP-severe group consisted of 14 patients (6 boys, 8 girls; mean age, 5.5 years; SD, 1.0 year) with the width of the alveolar cleft 4.0 mm or more at T1. The UCLP-mild group consisted of 13 patients (8 boys, 5 girls; mean age, 5.9 years; SD, 1.3 years) with the width of the alveolar cleft less than 4.0 mm at T1. No significant differences were observed in the 3 groups at 6 years of age (T2).
This study was approved by the Institutional Ethical Committee of Tokushima University Hospital.
A 3-dimensional measurement system (FN503; Mitutoyo, Kasugai, Aichi, Japan) was used for model analysis at T1 and T2. Reproducible reference points were defined according to those of Kramer et al ( Fig 1 ). A triaxial reference system was defined by an x-y plane containing the bilateral tuberosity points and the incisal point. The midpoint between both tuberosity points was the origin. All reference points were translated into 3-dimensional coordinates, and all measurements were calculated based on the coordinates.
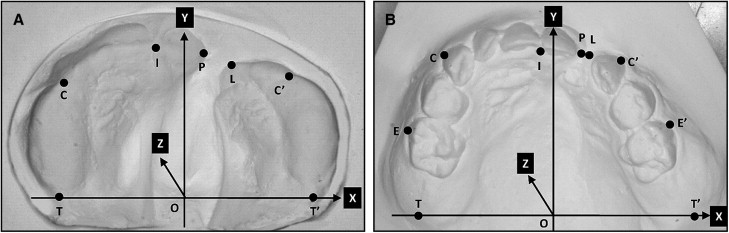
Three widths (P-L, width of the alveolar cleft; C-C′, anterior arch width; and T-T′, posterior arch width at the tuberosity points) were measured in the models at T1. Nine linear measurements (P-L, C-C′, T-T′, E-E′, posterior arch widths at the molars; I ⊥ TT′, arch depth; C-ITT′, alveolar height at the canine point on the major segment; C′-ITT′, alveolar height at the canine point on the minor segment; E-ITT′, alveolar height at the molar point on the major segment; and E′-ITT′, alveolar height at the molar point on the minor segment) and 4 angular measurements (CTT′, C′T′T, ITT′, and IT′T) were analyzed in the models at T2. The width of the alveolar cleft in the BCLP subjects was indicated as the mean value of both alveolar clefts. Alveolar heights were defined as the distances from the each reference points to the x-y plane.
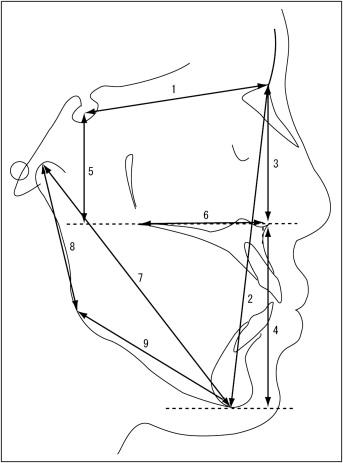
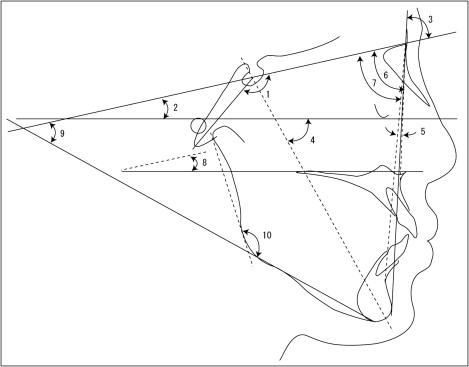
The lateral cephalograms at T2 were traced on acetate paper, and measurements of craniofacial morphology were made. Nine linear and 10 angular measurements were analyzed morphometrically and compared with the skeletal characteristics and the Japanese cephalometric norms ( Figs 2 and 3 ).
To eliminate interobserver error and ensure standardization, all measurements were made by 1 investigator (Y.T.). Intraobservation reliability was calculated by measuring all variables 2 weeks apart. A paired t test for the reproducibility of the measurements showed no significant differences between the variables measured 2 weeks apart, indicating that the variables were reproducible. The casual error was calculated according to Dahlberg’s formula (Se 2 ∑d 2 /2n), where Se 2 was the error variance, d was the difference between the repeated measurements, and n was the number of double measurements. According to the formula, the mean errors were 0.06 to 0.32 mm for the linear measurements and 0.22° to 0.54° for the angular measurements.
Statistical analysis
The Mann-Whitney U test or analysis of variance (ANOVA) and the Tukey-Kramer test were used to examine the model and cephalometric measurements. The Wilcoxon signed rank test was used to compare the differences of alveolar height between the minor and major segments at T2. The Spearman rank correlation was used to evaluate the correlations between the model measurements at T1 and the cephalometric variables at T2 in the UCLP patients. Probability less than 0.05 was considered significant. The analyses were carried out with statistical analysis software (StatView; SAS Institute, Cary, NC).
Results
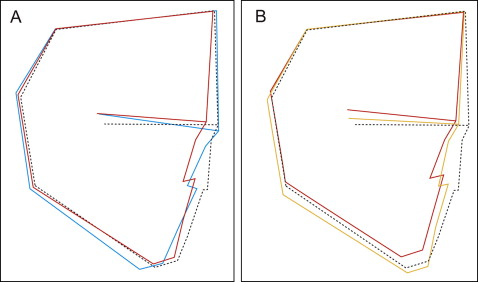
In the cephalometric analyses at T2, the maxillary length (PTM-ANS/PP) and the upper anterior facial height (N-PP) were significantly smaller ( P <0.05), and the facial angle was significantly greater in the UCLP group than in the BCLP group ( P <0.001; Fig 4 , A ; Table I ).
| Variable | Japanese norm ∗ | UCLP | BCLP | P value (UCLP vs BCLP) † | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Linear measurements (mm) | |||||||
| S-N | 62.6 | 2.5 | 62.2 | 3.1 | 63.9 | 2.8 | 0.1689 |
| N-Me | 104.7 | 3.8 | 102.4 | 6.4 | 106.1 | 6.3 | 0.1516 |
| N/PP | 44.9 | 1.8 | 43.6 | 2.9 | 46.5 | 2.2 | 0.0214 ‡ |
| Me/PP | 57.2 | 3.1 | 57.4 | 3.8 | 57.5 | 4.9 | 0.9373 |
| S/PP | 37.5 | 2.5 | 32.0 | 4.1 | 30.4 | 5.9 | 0.6944 |
| PTM-ANS/PP | 46.3 | 2.0 | 44.5 | 3.2 | 49.7 | 2.9 | 0.0006 § |
| Ar-Me | 87.2 | 3.7 | 85.5 | 5.2 | 84.8 | 5.5 | 0.7533 |
| Ar-Go | 36.7 | 2.4 | 37.1 | 3.6 | 38.3 | 3.5 | 0.3557 |
| Go-Me | 57.9 | 3.5 | 56.3 | 4.1 | 53.7 | 3.8 | 0.1354 |
| Angular measurements (°) | |||||||
| N-S-Ba | 130.7 | 4.7 | 134.1 | 4.5 | 134.6 | 4.9 | 0.8135 |
| FH-SN | 6.7 | 2.5 | 6.3 | 2.0 | 6.2 | 2.2 | 0.7983 |
| Facial angle | 81.6 | 1.8 | 81.1 | 2.9 | 77.9 | 5.0 | 0.0292 ‡ |
| Y-axis | 65.6 | 2.7 | 64.9 | 3.2 | 68.1 | 5.6 | 0.0620 |
| ANB | 4.9 | 2.0 | 0.5 | 2.5 | 5.1 | 5.8 | 0.0647 |
| SNA | 81.4 | 2.6 | 76.1 | 3.8 | 78.9 | 5.0 | 0.1207 |
| SNB | 76.4 | 2.6 | 75.6 | 3.2 | 73.8 | 5.0 | 0.2230 |
| PP-SN | 7.0 | 2.8 | 10.8 | 2.9 | 14.8 | 6.8 | 0.1206 |
| MP-SN | 40.2 | 4.1 | 37.7 | 5.1 | 41.3 | 7.1 | 0.2086 |
| Gonial angle | 130.0 | 4.7 | 128.3 | 5.7 | 130.9 | 6.2 | 0.2386 |
The mean values of the upper posterior facial height (S/PP) and the palatal plane angle (PP-SN) in both the BCLP and UCLP groups were out of the normal range, as previously reported. A short maxillary length with a small ANB angle because of a small SNA angle was observed in the UCLP group, and tendencies for greater maxillary length, enlarged y-axis, steeper mandibular plane (MP-SN), and longer total anterior facial height (N-Me) were shown in the BCLP group (these characteristics were compared with the normal values but not analyzed statistically; Fig 4 , A , and Table I ).
In the UCLP-mild group, the upper posterior facial height ( P <0.01), the total ( P <0.05) and lower ( P <0.01) anterior facial heights, and mandibular length (Ar-Me, P <0.01; Go-Me, P <0.05) were significantly greater, and the palatal plane angle was smaller than those in the UCLP-severe group ( P <0.05; Fig 4 , B ; Table II ).
| Variable | Japanese norm ∗ | UCLP-mild | UCLP-severe | P value UCLP-mild vs UCLP-severe † | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Linear measurements (mm) | |||||||
| S-N | 62.6 | 2.5 | 62.4 | 3.0 | 62.0 | 3.2 | 0.9613 |
| N-Me | 104.7 | 3.8 | 105.5 | 6.6 | 99.5 | 4.8 | 0.0101 ‡ |
| N/PP | 44.9 | 1.8 | 44.5 | 3.4 | 42.8 | 2.3 | 0.1089 |
| Me/PP | 57.2 | 3.1 | 59.5 | 3.4 | 55.4 | 3.1 | 0.0042 § |
| S/PP | 37.5 | 2.5 | 34.2 | 3.1 | 30.0 | 4.0 | 0.0066 § |
| PTM-ANS/PP | 46.3 | 2.0 | 44.6 | 3.3 | 44.3 | 3.1 | 0.8842 |
| Ar-Me | 87.2 | 3.7 | 87.9 | 5.1 | 83.3 | 4.2 | 0.0082 § |
| Ar-Go | 36.7 | 2.4 | 38.2 | 3.8 | 36.1 | 3.2 | 0.0848 |
| Go-Me | 57.9 | 3.5 | 57.9 | 4.1 | 54.7 | 3.6 | 0.0415 ‡ |
| Angular measurements (°) | |||||||
| N-S-Ba | 130.7 | 4.7 | 133.2 | 4.4 | 134.9 | 4.6 | 0.3436 |
| FH-SN | 6.7 | 2.5 | 6.4 | 2.4 | 6.2 | 1.6 | 0.8460 |
| Facial angle | 81.6 | 1.8 | 82.0 | 2.9 | 80.3 | 2.6 | 0.0892 |
| Y-axis | 65.6 | 2.7 | 65.0 | 3.5 | 64.8 | 3.0 | 0.9034 |
| ANB | 4.9 | 2.0 | 0.6 | 2.3 | 0.3 | 2.8 | 0.7157 |
| SNA | 81.4 | 2.6 | 76.7 | 2.6 | 75.4 | 4.7 | 0.4094 |
| SNB | 76.4 | 2.6 | 76.1 | 2.9 | 75.1 | 3.6 | 0.5765 |
| PP-SN | 7.0 | 2.8 | 9.5 | 1.7 | 12.0 | 3.3 | 0.0198 ‡ |
| MP-SN | 40.2 | 4.1 | 37.3 | 4.4 | 38.0 | 5.9 | 0.5440 |
| Gonial angle | 130.0 | 4.7 | 127.7 | 5.7 | 128.8 | 5.8 | 0.5441 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


