Bonding a flexible spiral wire retainer to the lingual surfaces of all 6 anterior mandibular teeth is a commonly used type of retention. Complications are rare but can be serious enough to produce biologic damage. This article presents a serious complication of a lingual flexible spiral wire retainer. Four years after the orthodontic treatment, a 20-year-old man sought treatment for a broken flexible spiral wire retainer. The clinical examination showed about 35° of buccal root torque of that tooth. A cone-beam computed tomography image showed that the root and the apex of the tooth were almost completely out of the bone on its buccal side. Surprisingly, the tooth’s vitality was preserved. The tooth was moved back, nearly to its original position; clinically, only a gingival recession remained. Orthodontists and dentists should be aware of possible complications of bonded retainers. Patients should be clearly informed how to detect problems at an early stage.
Bonded retainers in the mandible are today a standard of care. For example, Renkema et al found recently that 97% of all Dutch orthodontists use fixed retainers, usually flexible spiral wire retainers. In the mandible, 70% of the retainers were bonded to all 6 anterior teeth. Renkema et al showed also that flexible spiral wire retainers bonded to all anterior teeth demonstrate 90.5% efficacy 5 years after debonding. Although they are more effective than retainers bonded only to the mandibular canines, failures and adverse effects, such as torque differences of the incisors or an increased buccal canine inclination, can occur. When these complications are detected early, interceptive measures can prevent damage to periodontial tissues and bone. However, when they are found too late, they can be detrimental, and retreatment might become necessary. This article presents a severe complication of a flexible spiral wire retainer bonded to all mandibular anterior teeth.
Case report
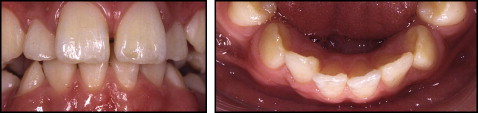
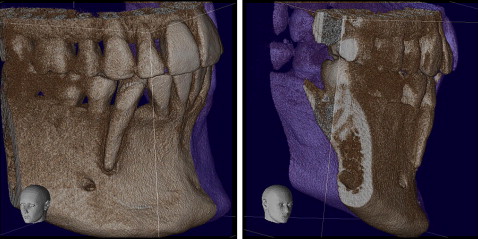
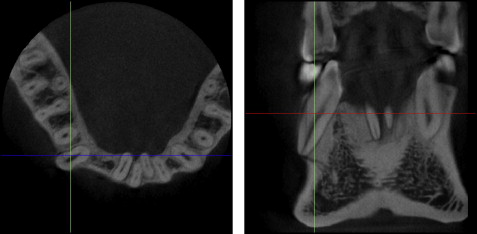
A 20-year-old man came to our clinic in Bern, Switzerland, 4 years after treatment because of a broken flexible spiral wire retainer between the mandibular right lateral incisor and canine. Initially, he had been treated with a straight-wire appliance because of congenitally missing premolars and misalignment of anterior teeth ( Fig 1 ). After treatment, a flexible spiral wire retainer had been bonded ( Fig 2 ). Subsequently, the patient was in orthodontic supervision for 2 more years. For the next 2 years, he did not show up for orthodontic checkups and did not consult a dentist. Although he had noticed an unusual position of his mandibular right canine, he asked for a check at our department only when his mandibular retainer broke. The clinical examination showed that the mandibular right canine was torqued about 35° buccally, with a strong lingual crown inclination and a recession of 1 mm on the buccal side ( Fig 3 ). The tooth was vital. The increased root torque was not present before or after the orthodontic treatment ( Figs 1 and 2 ). A 6 × 6-cm cone-beam computed tomography scan (3DX Accuitomo XYZ tomograph; Morita, Tokyo, Japan) was analyzed. The effective dose delivered to the patient by this device was within the range of 20 to 43 mSv, which is comparable with 1 to 2 panoramic x-rays. The root of the canine was almost completely out of the bone on its buccal side ( Fig 4 ). The apex was on the outer limit of the buccal cortical bone, but the tooth’s vitality was preserved; this means that the nerve and the vascular bundle had followed the apex ( Fig 5 ).


Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


