Introduction
The aim of this study was to evaluate differences in the maxillary sinus floor levels between adults with an anterior open bite and those without.
Methods
This retrospective study included 30 subjects: 15 adults with an anterior open bite (mean age, 21.5 ± 4.3 years) and 15 control subjects with normal occlusion (mean age, 21.7 ± 3.1 years). Cone-beam computed tomography and lateral cephalograms were analyzed before treatment.
Results
The open-bite group exhibited a significantly greater maxillary posterior alveolar height ( P <0.05). The craniocaudal heights of the maxillary sinus in the region between the first and second molars and between the second premolar and first molar were significantly greater in the open bite group (40.5 and 39.0 mm, respectively) than in the control group (36.7 and 34.7 mm, respectively; P <0.05 for both). The basal bone heights in the regions between the first and second molars, the second premolar and first molar, and the first and second premolars were significantly smaller in the open-bite group than in the control group ( P <0.001 for all).
Conclusions
Vertical pneumatization of the maxillary sinus floor in the region between the first and second molars and between the second premolar and first molar is greater in adults with an anterior open bite than in those without, whereas basal bone height in the maxillary posterior region is lower in the open-bite patients.
Highlights
- •
Open-bite patients had greater clockwise rotation of the mandibular plane.
- •
Open-bite patients had greater maxillary posterior alveolar height.
- •
Maxillary sinus height was greater in the open-bite group.
- •
Basal bone height was greater in the control group.
Open bite is associated with a vertical skeletal dysplasia in the jaws that arises below the cranial base, and it often requires surgical treatment. The etiology of open bite is associated with genetic and environmental factors that influence craniofacial traits. The skeletal and dentoalveolar characteristics of open bite include a long face with a steep mandibular plane angle, vertical growth with extrusion of posterior teeth in the maxillary arch, and an obtuse gonial angle.
The maxillary sinus floor comprises the maxillary alveolar process and the hard palate. The growth and development of the maxillary sinus are associated with maxillary structures and the maxillary posterior teeth, and are consequently influenced by any form of skeletal malocclusion. However, there are few reports on the relationship between the development of the maxillary sinus and malocclusion. Oktay compared differences in the maxillary sinus area among various skeletal profiles using panoramic radiography. Panoramic radiography has low resolution, and vertical and horizontal image magnifications and superimpositions of anatomic structures are problems. Therefore, cone-beam computed tomography (CBCT), which provides multiplanar views with a uniform and low magnification, should be used to overcome the limitations of panoramic radiography.
In adults, the maxillary sinus floor extends between adjacent teeth, creating elevations in the antral surface. This is considered an anatomic limitation that can adversely affect orthodontic tooth movement including intrusion or bodily movement. Oh et al reported that tooth movement using light continuous forces is necessary to move through the cortical bone of the maxillary sinus wall in adults. Nevertheless, unpredicted complications such as root resorption, pulp ischemia, alveolar bone loss, and perforation of the sinus membrane were found to occur while moving the teeth through the maxillary sinus in an animal study and a human biopsy study.
To our knowledge, no authors have investigated differences in the sinus floor levels between adult patients with an anterior open bite and those with normal occlusion using CBCT.
The aim of this study was to evaluate differences in the maxillary sinus floor levels between adults with an anterior open bite and those with a normal occlusion using CBCT. We tested the null hypothesis that there is no significant difference in the sinus floor level between subjects with and without an anterior open bite.
Material and methods
The study sample comprised 30 subjects with or without an anterior open bite whose dental records were retrospectively reviewed at the Departments of Oral and Maxillofacial Surgery and Orthodontics, College of Dentistry, Yonsei University, Seoul, Korea.
The inclusion criteria for the open-bite group were same ethnicity (Korean), age 18 years or older, anterior open bite greater than 1 mm, and mandibular plane angle (sella–nasion line to the mandibular plane) greater than 38°. The exclusion criteria were loss of at least 1 permanent tooth, severe craniofacial deformities such as cleft lip or palate, and a history of orthodontic treatment or orthognathic surgery.
All participants were required to exhibit good overall health conditions. Patients with serious medical conditions requiring hospitalization in the past 3 months were excluded to prevent any confounding effects of these conditions or medications on the results.
Of the 30 subjects, 15 (7 men, 8 women; mean age, 21.5 ± 4.3 years) fulfilled the abovementioned criteria and were enrolled in the open-bite group. All patients were scheduled for surgical correction of their anterior open bite. CBCT images were already obtained to establish a surgical treatment plan.
The remaining 15 patients (7 men, 8 women; mean age, 21.7 ± 3.1 years) had a normal occlusion and were a part of growth studies at The Institute of Craniofacial Deformity, College of Dentistry, Yonsei University, Seoul, Korea ( Table I ). This study conformed to the tenets of the Declaration of Helsinki for medical protocols and ethics and was approved by the institutional review board of Yonsei Dental Hospital.
| Normal occlusion (7 men, 8 women) Mean (SD) |
Anterior open bite (7 men, 8 women) Mean (SD) |
P value | |
|---|---|---|---|
| Age (y) | 21.7 (3.1) | 21.5 (4.3) | 0.367 ∗ |
| Range (y) | 19-28 | 18-31 | |
| ANB (°) | 2.7 (1.7) | 3.5 (4.1) | 0.538 † |
| SN-MP (°) | 33.7 (3.9) | 44.6 (3.8) | <0.001 † |
The lateral cephalograms were obtained (Cranex 3+ ceph; Soredex, Helsinki, Finland) before treatment and were digitized using V-ceph (version 5.5; Osstem, Seoul, Korea) by an observer (J.R.) who was blinded to the clinical status of the patients. In this study, we identified 4 anteroposterior and 11 vertical cephalometric measurements.
CBCT images were obtained with the subjects in a standard upright position (scanning time, 17 seconds; field of view, 20 × 17.9 cm; 80 kV(p); 5 mA; 0.39 voxel size) on the device (Alphard 3030h; Asahi Roentgen, Kyoto, Japan). The acquired data were imported into Invivo software (version 5.2; Anatomage, San Jose, Calif) in DICOM multifile format.
We selected the following reference planes on the CBCT images: axial plane, which passed through the anterior nasal spine in a direction parallel to the Frankfort horizontal plane; sagittal plane, which passed through the anterior nasal spine and the posterior nasal spine in a direction perpendicular to the axial plane; and coronal plane, which passed through the anterior nasal spine in a direction perpendicular to the axial and sagittal planes.
Then, measurements of the maxillary sinus dimensions were obtained, as described below, using previously reported methods on CBCT images.
- 1.
Linear measurements of the maxillary sinus height (craniocaudal height). The axial cut was oriented parallel to the maxillary posterior occlusal plane at the alveolar crest level, and the sagittal cut was oriented midway between the buccal and palatal cortices. For the coronal cut, the axial image was rotated until the orientation axis was perpendicular to the buccal cortex ( Fig 1 ).
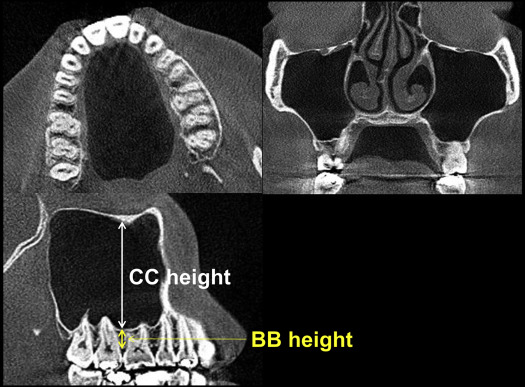
Fig 1 CBCT measurements of craniocaudal dimensions. CC height , Craniocaudal height; BB height , basal bone height. -
The same adjustments were repeated for the regions between the maxillary first and second molars, second premolar and first molar, and first and second premolars; the coronal cut was precisely oriented in the interdental regions. The maxillary sinus height was measured from the lowest point of the cortical boundary of the orbital floor to the lowest border of the cortical boundary of the sinus floor. In each of the 3 interdental areas, the basal bone height was measured from the lowest point of the cortical boundary of the sinus floor to the lower border of the alveolar crest. Eventually, 6 measurements were acquired as follows: craniocaudal height between the first and second molars, craniocaudal height between the second premolar and first molar, craniocaudal height between the first and second premolars, basal bone height between the first and second molars, basal height between the second premolar and first molar, and basal bone height between the first and second premolars.
- 2.
Linear measurements of the maxillary sinus depth (anteroposterior dimension) and width (mediolateral dimension). These measurements were obtained along the roots of the zygoma on each side. The orientation axis for the coronal cut was adjusted so that it precisely passed along the inferior cortical boundary of the zygoma root on both sides ( Fig 2 ). Measurements were repeated until the maximum anteroposterior and mediolateral dimensions were obtained.
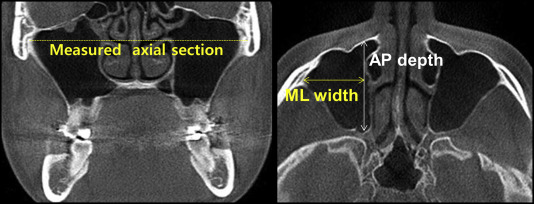
Fig 2 CBCT measurements of the anteroposterior ( AP ) depth and mediolateral ( ML ) width. Dotted line , measured axial section line. - 3.
Cross-sectional area measurements. The cross-sectional area of the maxillary sinus in the region between the maxillary second premolar and first molar was measured on a sagittal slice, because the software had a problem in reproducibility with regard to calculation of the total volume of the sinus from 3-dimensional reconstructive images ( Fig 3 ).
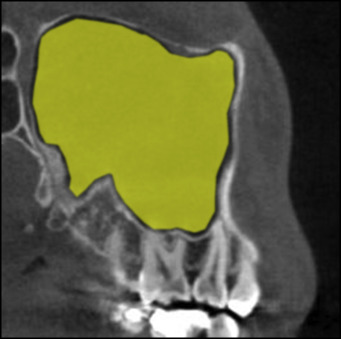
Fig 3 CBCT measurements of the cross-sectional area.
Reproducibility was evaluated by comparing measurements obtained during the initial and repeated examinations of randomly collected cephalometric and CBCT data from 20 patients over a 2-week interval by the same examiner (J.R.). The method error was calculated using Dahlberg’s formula. Errors ranged from 0.46 to 0.53 mm for linear measurements and from 0.81° to 0.89° for angular measurements; these values were not significant.
Statistical analysis
There were no significant differences in the CBCT measurements between the right and left sides; therefore, subsequent analyses were performed using the average values of the data for both sides. All statistical analyses were performed using SPSS software (version 21.0; IBM Korea, Seoul, Korea). The Shapiro-Wilk test was used to verify the normality of data distribution. Independent t tests and the Mann-Whitney U test were applied to detect significant differences in lateral cephalometric and CBCT measurements between the 2 groups. A P value of <0.05 was considered statistically significant.
Results
There were no significant differences in anteroposterior cephalometric measurements between the groups ( P >0.05 for all; Table II ). On the other hand, the open-bite group exhibited significantly greater clockwise rotation of the mandibular planes (SN-MP and FMA; P <0.001 for both) and greater maxillary posterior alveolar height (U6-PP; P = 0.013; Table II ).
| Measurement | Normal occlusion Mean (SD) |
Anterior open bite Mean (SD) |
P value |
|---|---|---|---|
| Anteroposterior | |||
| ANB (°) | 2.7 (1.7) | 3.5 (4.1) | 0.536 |
| Wits (mm) | −3.0 (2.2) | −3.7 (6.9) | 0.684 |
| Go-Me (mm) | 83.3 (6.0) | 80.2 (5.0) | 0.139 |
| Overjet (mm) | 2.5 (0.7) | 2.8 (3.9) | 0.798 |
| Vertical | |||
| SN-MP (°) | 33.7 (3.9) | 44.6 (3.8) | <0.001 |
| FMA (°) | 24.4 (3.9) | 35.4 (3.7) | <0.001 |
| SN-PP (°) | 11.2 (3.1) | 10.2 (3.0) | 0.393 |
| FH-PP (°) | 1.9 (2.3) | 1.0 (2.7) | 0.304 |
| PP-MP (°) | 22.5 (3.8) | 34.4 (4.1) | <0.001 |
| SN-OP (°) | 19.1 (5.3) | 23.4 (3.5) | 0.057 |
| AFH (mm) | 136.4 (6.4) | 140.4 (9.4) | 0.330 ∗ |
| PFH (mm) | 91.3 (7.0) | 82.6 (7.9) | 0.004 |
| Facial height ratio (%) | 66.8 (2.9) | 58.8 (2.5) | <0.001 |
| Overbite (mm) | 2.3 (1.0) | −2.0 (1.5) | <0.001 ∗ |
| U6-PP (mm) | 25.9 (2.4) | 28.3 (2.5) | 0.013 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


