Dental fluorosis manifests by too much ingestion of fluoride resulting in disturbances in enamel mineralization. The result is intrinsic discolorations in the maxillary and mandibular teeth with a poor esthetic appearance. In challenging cases, an esthetic result may be achieved only by a combination of techniques. This case report demonstrates a combination of modalities used to treat a patient presenting with atypical staining as a result of high-level exposure to ingested fluoride present in the drinking water as a child. Conservative treatment consisted of a combination of in-office bleaching to reduce the discoloration and porcelain veneers to create an esthetic result.
Key points
- •
Dental fluorosis manifests itself by too much ingestion of fluoride resulting in disturbances in enamel mineralization.
- •
The result is an intrinsic discoloration in the maxillary and mandibular teeth with a poor esthetic appearance.
- •
In challenging cases, an esthetic result may be achieved only by a combination of techniques.
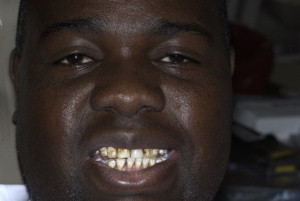
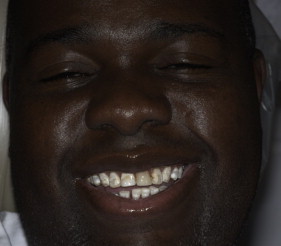
The patient was a 35-year-old African American man originally from Senegal, Africa who presented to New York University College of Dentistry with the chief complaint of discoloration of his anterior teeth and the desire to have white natural-looking and straight teeth ( Figs. 1 and 2 ). His chief complaint: “I need cosmetic work.”

Dental history
A full mouth series of radiographs were taken that displayed no carious lesions. Diagnostic casts were made and the American Academy of Cosmetic Dentistry series of photographs were taken. Teeth #14, #19, and #30 were missing. A dental implant was proposed for future placement in the #30 position. The space was too narrow in the other positions. A class I malocclusion with bimaxillary protrusion was present. This condition is characterized by protrusive and proclined upper and lower incisors and an increased procumbency of the lips.
A New York University College of Dentistry Smile Evaluation Form was completed. A clinical examination was performed and the basic restorative work subsequently completed. Periodontal examination revealed the need for scaling and root planing to achieve desired gingival health. The periodontal status showed local and generalized recession. Periodontal probing and charting revealed sulcus depth was within normal limits but mild gingivitis was present.
Treatment plan and sequencing
The patient’s esthetic problem was caused by fluorosis. Treatment options included bleaching; microabrasion; direct or indirect composite resin; porcelain veneers; and all ceramic crowns, such as e.max (Ivoclar Vivadent, Amherst, NY) with some opacity to mask the discoloration but still allow an esthetic restoration by combining an opaque core with an esthetic veneer of feldspathic porcelain. The conservative treatment of bleaching in conjunction with feldspathic veneers was selected.
Prognosis
The depth of the staining could not be ascertained. Teeth bleaching was used to reduce the discoloration of the teeth before preparation and therefore the necessity for more opaque veneers. This would allow a more natural appearance of the final veneered teeth and allowing for an excellent prognosis.
Treatment sequencing
Periodontal Considerations
Scaling and root planing resulted in the resolution of the patient’s gingivitis. A healthy periodontium created the appropriate environment for the restorative phase of treatment. The gingival zeniths were determined to be in the correct position and no surgical intervention was required.
Restorative Considerations
The initial phase requires in-office bleaching (Philips Zoom Light-Activated Whitening System [Philips Oral Healthcare, Stamford, CT]). An initial shade was taken to document the change (see Fig. 2 ; and Fig. 3 ). Three bleaching sessions were performed with 15-minute cycles in the same visit ( Figs. 4 and 5 ).


Feldspathic porcelain veneers on eight upper teeth were suggested subsequent to the bleaching. However, financial constraints permitted only teeth #6 to #11 to be treated. Bleaching was performed on the lower arch to improve their appearance and an acceptable result was accomplished. The concept of golden proportion without any spacing was used to guide the wax-up and mock-up before preparation for the porcelain veneers.
The preparations were done with a diamond chamfer bur and guided with a preparation guide to have a controlled reduction ( Fig. 6 ). The stains were taken out when prepared with a 0.5-mm facial reduction. In this case the staining was not deep, although unknown before preparation. If the staining was deeper, a deeper preparation would have been required.

Final impressions were taken with Dentsply Reprosil polyvinyl siloxane (Dentsply Caulk, Milford, DE) and the resulting stone model was evaluated for adequate preparation. Provisionals were created from the wax-up using Luxatemp Shade A-1 (DMG America, Englewood, NJ), which was placed into a putty matrix.
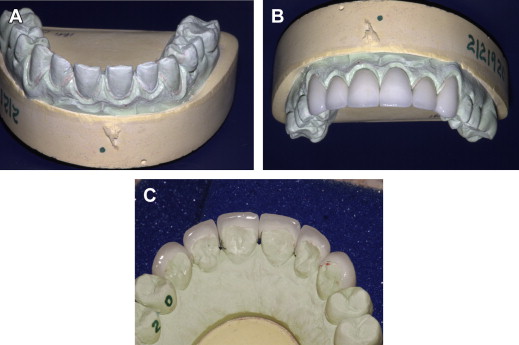
The laboratory was supplied with the study models of the wax-up. Feldspathic porcelain was used for the veneers to obtain the most esthetic result. Opaque porcelain was ordered to block-out the discoloration of the color of the teeth.
When the case came back it was placed onto the model to check for accuracy before the patient’s appointment Fig. 7 .