Introduction
In this study, we evaluated the reproducibility of natural head position for pitch and roll acquired using 3 methods.
Methods
The participants were 30 Chinese adults (ages, 23-28 years) who had normal occlusion with no history of orthodontic therapy, maxillofacial trauma, or surgery. The natural head position was acquired using the self-balanced, mirror, and estimated positions, which were performed in duplicate and repeated after 1 week. Three-dimensional photographs were recorded with a horizontal laser line projected onto the face. The laser lines were observed by registering the repeated 3-dimensional photographs. The roll and pitch of the head orientation were measured with a digital ruler. Reproducibility was calculated using Dahlberg’s formula and the Bland–Altman method.
Results
The reproducibility values calculated with Dahlberg’s formula were 1.51°, 1.2°, and 0.99° for pitch, and 0.78°, 0.76°, and 0.41° for roll in the self-balanced, mirror, and estimated positions, respectively.
Conclusions
The 3 methods are reproducible for both pitch and roll, and the estimated position showed the best reproducibility among these methods. This indicates that the estimated position could be used for acquiring the reference plane in preoperative planning for orthognathic surgery.
Highlights
- •
We recorded natural head position (NHP) with horizontal laser level and 3dMDface imaging system.
- •
NHP was studied in both the sagittal and coronal planes.
- •
Three ways to acquire NHP—self-balanced, mirror, and estimated positions—were compared.
- •
The estimated position has the best reproducibility.
Orthognathic surgery is a main treatment method for problems with occlusion. With the development of computer-based technologies, more medical centers are beginning to use computer-aided surgical simulations for preoperative planning. Since the reference plane plays a crucial role in the preoperative design, the choice of reference plane has received much attention, particularly the Frankfort horizontal plane (FH plane) and the true horizontal plane, which is based on the natural head position (NHP).
The FH plane has become the most important reference plane since it was introduced in an orthodontic study in the 1880s. It is considered that the FH plane in most people is parallel to the horizontal plane when the head is in the natural position. However, research has indicated that an obvious deviation of the FH plane from the horizontal is common, with the deviations of the angle formed by the FH plane and the true vertical plane ranging from 76.3° to 120.7° (mean, 89.27°; standard deviation [SD], 5.02°). This deviation must be considered if the FH plane is selected as the reference plane when planning treatment. In addition, it is difficult to locate the left and right orbitales and porions on the same plane, so it would be difficult to choose the 3 points to define the FH plane. An alternative method is to use the midpoint of the 2 points, but it is also difficult to choose these 2 points.
Because of these shortcomings of the FH plane, the true horizontal plane based on the NHP is becoming more popular. Only when the NHP is acquired can the true horizontal plane be used as the reference plane. Two methods have been widely used to acquire the NHP: the self-balanced position and the mirror position. It has also been reported that the head position could be reproduced with less variation when corrections are made by the doctor, especially for patients with a Class II or Class III malocclusion ; this position is referred to as the estimated position in this article. Some authors have compared the reproducibility of the 3 methods of NHP in the sagittal plane (pitch), but no studies have compared the reproducibility of the 3 NHP methods in the coronal plane (roll).
In this study, we aimed to compare the reproducibility of NHP for pitch and roll acquired in the self-balanced, mirror, and estimated positions to identify a practical, reproducible position for preoperative digital design in orthognathic surgery.
Material and methods
Thirty Chinese adults (15 women, 15 men) with normal occlusion were included in this study. Their ages ranged from 23 to 28 years (mean, 25.2 years; SD, 1.56 years). Those with a history of orthodontic therapy, maxillofacial trauma or surgery, or any disease of the motor system or vision system were excluded. If the subject had a cold with nasal obstruction at the NHP recording, it was delayed until the subject recovered.
This study was approved by the institutional review board of the Peking University School of Stomatology, Beijing, China (number PKUSSIRB-201413039). Informed consent was obtained from all participants before the study.
NHP was obtained in 3 ways: self-balanced position (position 1), mirror position (position 2), and estimated position (position 3). In the self-balanced position, each subject was first asked to sit upright with both hands on the thighs. Then, the subject tilted his or her head and decreased the amplitude until he or she was in a comfortable position, which was considered as the self-balanced position. In the mirror position, the subjects were asked to sit upright, tilt the head and decrease the amplitude, and then look at their eyes in a mirror (85 × 120 cm) located 150 cm in front of them. For acquiring the estimated position, the mirror position was adjusted by the same researcher (K.T.) for all participants. The standard criteria for the estimated position were that neither flexion nor extension of the head was observed in pitch and no obvious tilt of the head to the left or right was observed in roll.
The laser level SW902 (Saiwei, Shanghai, China) and the 3dMDface imaging system (3dMD, Atlanta, Ga) were used to record the NHP ( Fig 1 ). According to the manufacturer’s handbook, the wavelength of the laser was 635 nm, with a horizontal accuracy of 0.2 mm per 1 m. The recording procedure was as follows.
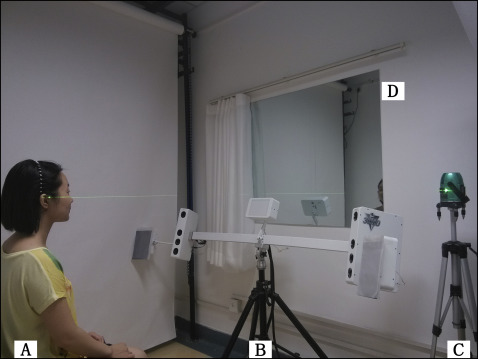
First, with the subject sitting straight, the height of the laser level was adjusted so that it could project a horizontal laser line onto the participant’s face within the area from the nasal apex to the infraorbital margin. Then, the center flashlight of the 3dMDface imaging system was turned off so that the laser line appeared more clearly on the obtained images. After these settings, the subject was asked to position the head in the NHP, and then the laser level was turned on to project the horizontal laser line, and the shutter of the 3dMDface imaging system was pressed to record the 3-dimensional (3D) photograph of the face.
To reduce any error that might be caused by a slight shaking of the subject’s head, all 3 positions were acquired in duplicate for all subjects (in the order of self-balanced, mirror, and estimated positions [T1]). The subjects were asked to rest and walk around for about 5 minutes between the recording of positions 1 and 2, and between the recording of positions 2 and 3. This procedure was repeated after 1 week (T2). Eventually, a total of 12 photographs were taken of each subject.
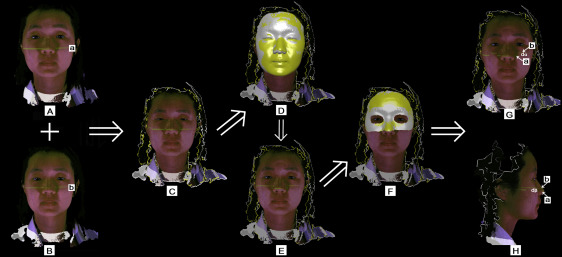
To evaluate the changes in head position, the 3D photographs of the same subjects were registered by the same researcher (K.T.) in the 3dMDpatient software (3dMD; Fig 2 ). The self-balanced position is shown here to illustrate the registration procedure. There were 4 photographs of the self-balanced position for each subject. These photographs were registered together in 3 steps. First, the 3D photographs were registered by surface registration based on the whole surfaces ( Fig 2 , C ). Second, the whole face region was selected, and surface registration based on the selected region was performed ( Fig 2 , D and E ). Although all subjects were asked to relax their faces, there might have been some differences around the mouth and eyes between the photographs. Therefore, in the third step we cleared the selected whole face region, reselected a relatively stable region, and finally performed another fine registration based on that region ( Fig 2 , F ). Subsequently, the differences between the laser lines could be observed ( Fig 2 , G and H ). The same registration procedure was performed for the mirror and the estimated positions.
For the measurement of NHP, the DWRule (version 1.0; Dowell, Beijing, China) was used to measure the angles, with an accuracy of 0.01°. When the ruler was rotated away from the horizontal, the rotation angle could be displayed automatically ( Fig 3 ). The self-balanced position is shown here to illustrate the measuring procedure.
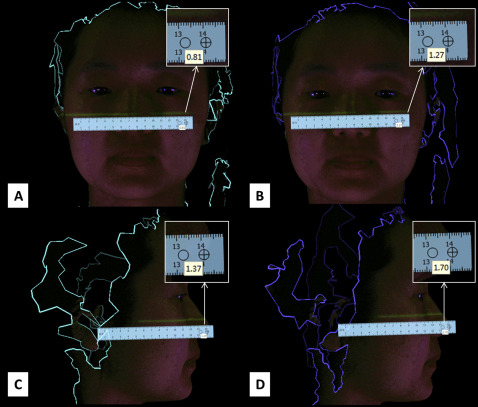
The registered 3D photographs were locked together and rotated to display the frontal view, and the inner canthus line was made horizontal to the axial plane in the 3dMDpatient software ( Fig 2 , G ). Then, we displayed the 3D photographs one by one and took a screenshot of each photograph in the frontal view. During this screenshot procedure, the 3D photographs could not be rotated. After all the screenshots of the frontal views had been taken, the right lateral view of the 3D photographs was displayed ( Fig 2 , H ). Then, all 3D photographs were hidden again. This time, screenshots of each 3D photograph were taken in the right lateral view after displaying them one by one. During this procedure, no rotation of the 3D photographs could occur. All screenshots were saved as .jpg files. After this procedure, the frontal and right lateral views of all 3D photographs in 1 coordinate system could be recorded. Thus, the angle measured by the DWRuler between the laser line and the horizontal line of the screen represented the roll of the head orientation (in the frontal view, Fig 3 , A and B ) and the pitch of the head orientation (in the right lateral view, Fig 3 , C and D ).
All angles were measured 3 times at an interval of at least 3 days to reduce measurement error. All measurements were made by the same researcher (K.T). With regard to each position at each time (T1 or T2), 2 photographs were taken; a total of 6 measurements were obtained for both roll and pitch. The mean value of these 6 angles was calculated as the final angle to represent the roll or pitch angle for each position at each time.
The 3D photographs of 15 subjects (8 men, 7 women) were selected randomly to test the reliability of the measurements. The angles mentioned above were measured by 2 researchers (K.T. and another). Each researcher repeated the measurements 3 times at an interval of at least 3 days. The SPSS statistical package (version 13.0; SPSS, Chicago, Ill) was used to calculate the intraclass correlation coefficient (ICC) to estimate the reliability of the measurements.
The reproducibility of NHP was evaluated for pitch and roll separately. The reproducibility was calculated for each method separately using Dahlberg’s formula (methoderror=√∑d2i/2n)
( method error = ∑ d i 2 / 2 n )
. In the formula, d i ( d α for roll and d β for pitch; Fig 2 , G and H ) was the difference between the initial and repeated photographs (T1 and T2) for the same position, and n was the sample size. Excel (version 2010; Microsoft, Redmond, Wash) was used for this calculation.
To make it more intuitive, the method of Bland and Altman was also used to evaluate the reproducibility. The 1-sample Kolmogorov-Smirnov test was used to test normality, and the assumption of normal distribution could not be rejected. Software (version 15.2.2; MedCalc, Ostend, Belgium) was used to perform the Bland-Altman analysis.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


