The use of cone beam CT (CBCT) is common among dentists and dental specialists in North America and the world. The regions of interest captured by these machines vary in size and applications are numerous. If using the image data from this modality, clinicians are obligated to examine the entire volume and to understand and recognize all the anatomy in the head and neck region that can be portrayed and any abnormalities detected in otherwise normal surroundings. This article attempts to identify common entities found in the anatomic regions captured in a CBCT volume and those common abnormalities that must be referred.
Key points
- •
It is the responsibility of health care providers to acquire information data from patients to best determine the health status of patients and if treatment is indicated and to provide a basis for informed patient consent.
- •
The use of CBCT for dental treatment planning poses a situation in which the additional data in the acquired image volume that are outside of the scope of the primary dental concern could detect systemic conditions that possibly have a direct influence on the overall health and longevity of a patient.
- •
Patients can make informed decisions about their health or dental care and treatment. The CBCT report becomes a component of the informed consent standard of care.
- •
Who provides the report may not be as important as whether or not a report is actually performed.
- •
The quality, accuracy, and use of a report are subject to medicolegal scrutiny, and knowledge of such issues determine whether or not a primary provider or a secondary radiology reader evaluates the image data and issues the final report.
Introduction
As in any disruptive technology introduced to a profession, the education lags far behind the technological advance. This is especially true of cone beam imaging. Dentists and dental professionals are quick to grasp the advantages and applications of using cone beam technology but, once adopted, often make the following statements:
These images are great, but what am I looking at? and
Where can I get more information on interpreting the scan?
Unfortunately, there is no easy answer and no quick way for dentists to re-educate themselves. Understanding CBCT takes time and effort and even some guidance. Manufacturers, also quick to understand the popularity of this technology, often fail to provide even the basic education that is necessary so that clinicians do not inadvertently cause harm to patients. Reporting the findings in a CBCT volume is probably the most essential process in the total diagnostic evaluation of a patient, even if it is something as simple as implant planning. Dentists and dental specialists must not be caught in the trap of only looking at the data they are interested in, such as an impacted tooth or implant site evaluation or characterization of some pathologic entity that they found in another radiograph. They must examine all the data in the scan and must do so in a systematic and somewhat regimented fashion.
This article is designed to help clinicians understand the process and expose them to the methodology the authors use and a software tool the authors developed to help dentists completely examine and report all findings in a scan and take the appropriate next steps when the findings dictate additional action, such as referral to a dental specialist or a colleague in the medical profession. This methodical, diagnostic approach is for precise communication with the referring clientele. When the authors examine and report findings in a 3-D scan, they are looking for occult pathology, that is, anything that might have an impact on a patient’s health that the dentist needs to know about and sometimes takes action on. The authors cannot afford to miss an important finding or fail to communicate these findings to referring clinicians. For those individuals to examine their own data, this is also true. No clinician would be in trouble for misdiagnosing a condition or problem, but that same clinician is definitely placing himself or herself at risk for not examining the volume for these occult findings. The authors support each of the areas of discussion with cases from their files to illustrate the common and not so common findings discovered in cone beam scans and know this will be helpful to all dentists.
Introduction
As in any disruptive technology introduced to a profession, the education lags far behind the technological advance. This is especially true of cone beam imaging. Dentists and dental professionals are quick to grasp the advantages and applications of using cone beam technology but, once adopted, often make the following statements:
These images are great, but what am I looking at? and
Where can I get more information on interpreting the scan?
Unfortunately, there is no easy answer and no quick way for dentists to re-educate themselves. Understanding CBCT takes time and effort and even some guidance. Manufacturers, also quick to understand the popularity of this technology, often fail to provide even the basic education that is necessary so that clinicians do not inadvertently cause harm to patients. Reporting the findings in a CBCT volume is probably the most essential process in the total diagnostic evaluation of a patient, even if it is something as simple as implant planning. Dentists and dental specialists must not be caught in the trap of only looking at the data they are interested in, such as an impacted tooth or implant site evaluation or characterization of some pathologic entity that they found in another radiograph. They must examine all the data in the scan and must do so in a systematic and somewhat regimented fashion.
This article is designed to help clinicians understand the process and expose them to the methodology the authors use and a software tool the authors developed to help dentists completely examine and report all findings in a scan and take the appropriate next steps when the findings dictate additional action, such as referral to a dental specialist or a colleague in the medical profession. This methodical, diagnostic approach is for precise communication with the referring clientele. When the authors examine and report findings in a 3-D scan, they are looking for occult pathology, that is, anything that might have an impact on a patient’s health that the dentist needs to know about and sometimes takes action on. The authors cannot afford to miss an important finding or fail to communicate these findings to referring clinicians. For those individuals to examine their own data, this is also true. No clinician would be in trouble for misdiagnosing a condition or problem, but that same clinician is definitely placing himself or herself at risk for not examining the volume for these occult findings. The authors support each of the areas of discussion with cases from their files to illustrate the common and not so common findings discovered in cone beam scans and know this will be helpful to all dentists.
Systematic review of image database
- A.
Confounds: axial sections, smaller field-of-view (FOV) confusion, and anatomy outside the dentists’ comfort zone
- B.
Suggested method of review
Confounds—Some of the Obstacles to Overcome When Examining the Volume
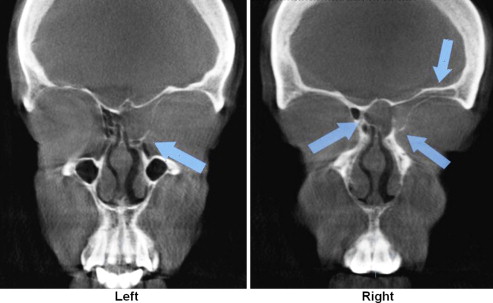
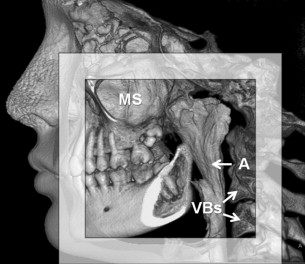
Most dentists carefully and systematically examine bitewings for interproximal carious lesions; periapical radiographs for signs of bone loss or apical problems; or panoramic images for dental, temporomandibular joint (TMJ), and sinus problems. Through training and clinical experience, they develop their own approaches for a systematic review of the radiographic images. All these images that they were taught to look at, however, are oriented in a sagittal anatomic plane of section. That is, all these images of a patient are looked at from the side. Cone beam data sets significantly alter this paradigm. The coronal and axial anatomic planes of section can also be viewed. Although the coronal plane is understandable, the axial plane of section is a significant departure from the dental paradigm. Fig. 1 demonstrates a finding in the 3 planes of section.
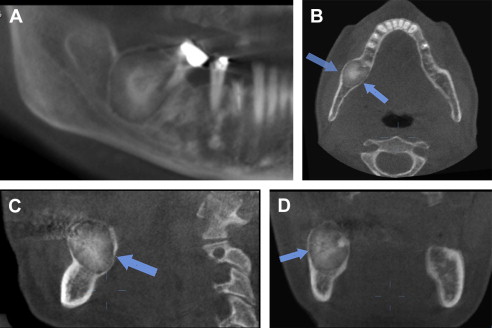
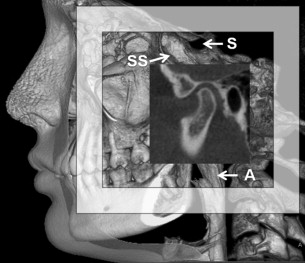
In addition to the confound of these new planes of orientation, dentists were also informed by the manufacturers that a smaller FOV represented less diagnostic responsibility. Unfortunately, although this is true in most cases, an axial image from a limited field cone beam machine, such as the unilateral capture of the TMJ condyle, when seen in a axial orientation, is confusing. Fig. 2 illustrates this point.
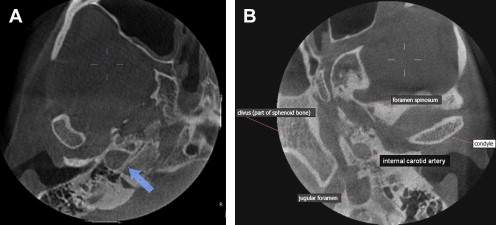
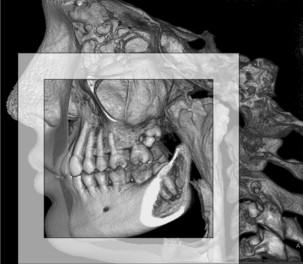
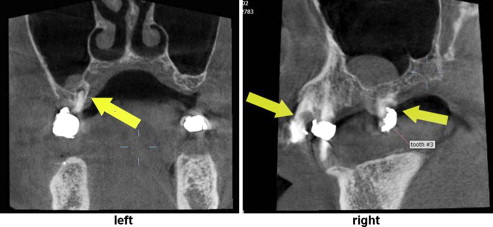
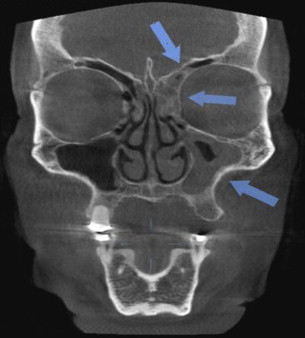
Another obstacle dentists must overcome is educating themselves to look beyond the dental bases to anatomic regions with which they are less familiar. These include the cranial vault, the paranasal sinuses, the nasal cavity, the airway, and the cervical spine. Those dentists thinking that a smaller FOV relieves them of all this responsibility are wrong. Moving the area of capture with a small volume sometimes captures pathology in the anatomic areas listed previously. Figs. 3–5 illustrate this concept.
A Suggested Method for Scan Review
Even within the medical radiology community there continues debate between the utility of a structured radiology report versus a narrative report. According to Dr Curtis P. Langlotz, Professor and Vice Chair for Informatics in the Department of Radiology at the University of Pennsylvania Health System, approximately 98% of medical radiology residents received no formal training in radiology reporting. Most, apparently (78%), learned the process from a fellow resident. Concerning a structured report, however, he was quoted in the online journal, Diagnostic Imaging :
the purpose of structured reporting is to communicate to colleagues in a clear way and to make that reported information accessible to the software applications that are meant to improve communication.
It seems, then, that the adoption of a formal reporting system in the dental profession that helps dentists and dental specialists review their CBCT volumes competently is desirable. Recently, the authors, in combination with a large cone beam dental software company, released reporting software, called EasyRiter , in an attempt to fill this void. The model for the software was developed from their approach to provide structured, interpretive reports for their clinician/clients. So that they themselves ensure that they examine every portion of the volume, the following anatomic regions, when present, are always examined each time in the same fashion to determine abnormal conditions or occult pathology to report to their referring clients:
- 1.
Paranasal sinuses
- 2.
Nasal cavity
- 3.
Airway
- 4.
Cervical structures
- 5.
TMJs
- 6.
Dental findings
- 7.
Other findings
From any abnormal findings discovered, clinical impressions, differential diagnoses, and medical recommendations are provided to a referring dentist supported by the images embedded in the report. In addition, when necessary, citations about the import conditions are included to help assist dentists with their referral to an appropriate medical specialist. A sample report appears in [CR] .
According to Wilcox, failure to communicate clearly and effectively to a referring health care provider is 1 of the 3 most common reasons for malpractice suits. The authors agree with this. Wilcox further asserts that the report must be understandable to both the patient and referring clinician. Many of the authors’ clients use the reports chairside to present these significant findings to a patient. Unlike medical radiology reports, embedding the pertinent images in the report allows a dentist to visually display to patients a significant finding. The authors think that the use of the formatted report allows clearly communicating the importance of the findings to the clinician, who then subsequently discusses these findings with patients. One example of such a report is in Appendix 2 .
Common findings in anatomic regions in CBCT data sets by anatomic region
Paranasal Sinuses
As reported in a previous article by Parks, the paranasal sinuses include the frontal, sphenoid bone, and maxillary sinuses as well as the ethmoid air cell complex. Most dentists are familiar with inflammatory changes that might occur in the maxillary sinuses. Common changes in the maxillary sinuses include mucosal thickening, mucus retention phenomenon (antral pseudocyst), and, although less common, the occasional antrolith. When the inflammatory changes seen in the maxillary sinus are extensive, often the other paranasal sinus spaces are involved. Figs. 6–9 show examples of common changes.
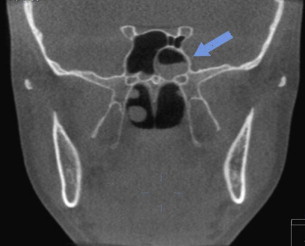

It is important to consider the possibility of inflammatory change in the other paranasal spaces when significant portions of the maxillary antra are involved. In some cases, this may mean immediate referral to a primary care provider and/or an otolaryngologist for clinical and endoscopic evaluation of all the paranasal sinuses, even if only a portion of the maxillary antra is visualized in the limited FOV scan.
More rarely, sinus mucoceles (destructive inflammatory lesions, unlike those of the salivary gland type) can also develop in the paranasal sinus spaces; these occur much less frequently than the mucus retention phenomenon (antral pseudocyst) in the maxillary sinuses but when they occur are more commonly located in the frontal and sphenoid sinuses as well as the ethmoid air cell complex. Fig. 10 shows an example of a mucocele.