Introduction
The aims of this study were to compare 3-dimensional cone-beam computed tomography (CBCT) images of patients with unilaterally impacted canines and to determine the possible radiographic factors for prediction of maxillary canine impactions.
Methods
The sample consisted of 65 patients ranging in age from 9.6 to 13.8 years. The patients comprised 43 girls and 22 boys, with a mean age of 12.1 years and a median age of 12.2 years (±SD 1.23 years). Of the impacted maxillary canines, 32 were located on the right side and 33 on the left side. CBCT radiography was available for all patients. The diagnosis of a unilaterally impacted canine was determined from the patients’ dental records as a unilateral failure of the canine to erupt at its appropriate site in the dental arch in contrast to normal eruption of the contralateral side. Radiographic follow-up assessment to identify unilateral impaction was performed for 1 year. The radiographic variables generated and the specific features investigated were collected with 3-dimensional CBCT imaging and compared between the impacted and the contralateral maxillary canines.
Results
Statistically significant differences were found between the impacted and nonimpacted canines. Based on these results, clinical relevance and correlations among the variables—canine rotation, canine crown position, canine cusp tip to the midline and to the occlusal plane, canine angle to the midline, and canine angle to the lateral incisor—were considered as variables in a multivariable prediction model. A prediction model using CBCT for canine impaction was established (area under the curve, 0.965; 95% confidence interval, 0.936 to 0.995). Canine crown position, canine cusp tip to the occlusal plane, and canine angulation to the lateral incisor were the relevant predictors in this model.
Conclusions
Prediction of canine impaction based on CBCT was excellent. The probability of canine impaction obtained from the prediction model can help orthodontists to define the optimal intervention method.
Highlights
- •
Prediction of the probability of canine impaction based on CBCT was excellent.
- •
Angulation to lateral incisor, cusp tip to occlusal plane, and crown position were the predictors.
- •
The prediction model can help orthodontists to define the optimal intervention method.
Impacted maxillary canines are a common problem in orthodontic practice, with up to 5% of patients seeking orthodontic treatment. According to the literature, the incidence of female patients with maxillary canine impaction shows a strong prevalence and has been well documented. Several local factors have been hypothesized for maxillary canine impaction, such as a narrow maxillary arch or a Class II Division 2 malocclusion. A possible genetic origin for palatally displaced canines has also been indicated. Palatally impacted canines are usually associated with other dental anomalies, such as congenital absence of the lateral incisors or the second premolars, and peg-shaped lateral incisors. An impacted canine may cause root resorption of adjacent teeth, particularly the lateral incisor. Several studies have reported that incisor root resorption is more common in female patients than in males, with wide variations in the severity among different racial populations. Incisor root resorption is asymptomatic and usually diagnosed late in relation to the patient’s age and the severity of resorption.
The treatment of impacted canines is multidisciplinary and associated with prolonged treatment time and increased costs. The choice of treatment is influenced by several factors, such as canine location, severity of impaction, patient age, and other patient considerations. Interceptive orthodontic treatment is often the first approach in growing persons for guiding the canine into a normal position and preventing tooth impaction. The treatment sometimes consists of removal of the maxillary deciduous canines or is combined with creating spaces in the dental arch by distalization, extraction of the maxillary deciduous first molar, or maxillary expansion. However, it has been found that extraction of only the deciduous canine is not effective. Surgical exposure of the impacted canine is essential when interceptive treatment fails, usually requiring a combination of surgical and orthodontic interventions to bring the canine successfully into the dental arch. Furthermore, older patients with impacted canines require more time and are more difficult to treat than younger patients. A novel 3-dimensional (3D) classification system (KPG index) was developed as a method to classify and estimate the difficulty of treatment of impacted maxillary canines using cone-beam computed tomography (CBCT) images, without multiple measurements of angles and distances. The reliability and the repeatability of this index have been proven in other studies to be easy and efficient. However, the efficacy in estimating treatment time based on the difficulty score is always difficult and still unknown.
Early prediction and early diagnosis of impaction with 2-dimensional (2D) radiographs remains problematic. It is challenging to distinguish structures based on conventional 2D radiographs, which often lead to misinterpretations. CBCT images, by their nature, have significant advantages over 2D images. When a 3D view is available, many diagnostic issues related to impacted canines can be easily answered. Potential complications of canine impaction include the need for CBCT images so that the orthodontist can understand the development of impaction and normal eruption. Several studies have investigated the possible predictors of canine impaction and orthodontic treatment choices with 2D radiographs. Therefore, the aims of this study were to compare 3D CBCT images of unilaterally impacted canines with the normal contralateral sides, and to detect possible radiographic factors involved in maxillary canine impaction.
Material and methods
This investigation was based on the radiographic records of patients who were referred for CBCT images. All patients were nonsyndromic and were selected if they had a unilaterally impacted maxillary canine. The sample consisted of 65 patients ranging in age from 9.6 to 13.8 years. They included 43 girls and 22 boys, with a mean age of 12.1 years and a median age of 12.2 years (±SD, 1.23 years). Of the impacted maxillary canines, 32 were located on the right side and 33 on the left side. The diagnosis of unilaterally impacted canine was determined from the patients’ dental records as a failure of the canine to erupt at its appropriate site in the dental arch in contrast to normal eruption of the contralateral side. Radiographic follow-up assessment to identify unilateral impaction was performed for 1 year. The study protocol was approved by the medical ethics committee of the University of Leuven in Belgium (approval numbers B32220083749, S50910).
All patients had a CBCT scan with either of 2 CBCT systems. The first involved a 3D Accuitomo-XYZ Slice View Tomograph (J. Morita Corp, Kyoto, Japan) with a voxel size of 0.125 mm (field of view, 30 × 40 mm). Parameters included tube voltage of 80 kV, tube current of 3 mA, and scanning time of 18 seconds. The second system was a Scanora 3D CBCT (Soredex, Tuusula, Finland) with a voxel size of 0.2 mm (field of view, 75 × 100 mm), tube voltage of 85 kV, current of 10 mA, and scanning time of 3.7 seconds.
The protocol included evaluation of variables related to specific features obtained from the radiographic records, which were analyzed by 1 investigator (A.A.). The variables were categorized as the following.
Canine-related variables
- 1.
Crowding in the maxillary anterior region.
- 2.
The maxillary deciduous canine was assigned to 1 of 3 categories: missing tooth, where the deciduous canine had been extracted; present without root resorption; or present with root resorption.
- 3.
Canine development was assigned to 1 of 4 categories based on root development: complete development, 75% of the root developed, 50% of the root developed, and 25% of the root developed.
- 4.
Canine apex: open, closed, or dilacerated.
- 5.
Detection of abnormalities, such as canine root resorption, mesiodens, peg-shaped lateral incisor, agenesis of permanent teeth, and impaction of other permanent teeth.
- 6.
Canine rotation: mesiovestibular, distovestibular, mesiopalatal, or distopalatal.
- 7.
Canine position in relation to adjacent teeth was determined from the CBCT images as palatal, buccal, or in the line of the arch.
- 8.
Type of canine impaction was assigned to 1 of 3 categories: no impaction; vertical impaction, if the impacted canine was vertically inclined and covered with soft or bony tissue; and horizontal impaction, if the impacted canine was horizontally inclined and covered with soft or bony tissue.
- 9.
The roots of the first premolar were categorized as single root, separated roots, or fused roots.
- 10.
Anterior apical area was recorded as optimal, small, or severe.
- 11.
Contact relationship between the canine and adjacent teeth was assigned to 1 of 2 categories based on the categories suggested by Ericson et al : contact, if the distance between the crown of the maxillary permanent canine and adjacent incisors is less than 1 mm; and no contact, if the distance between the crown of the maxillary permanent canine and adjacent incisors is more than 1 mm.
Linear measurements in millimeters
- 1.
Canine cusp tip to the midline was measured in the axial view ( Fig 1 , A ).
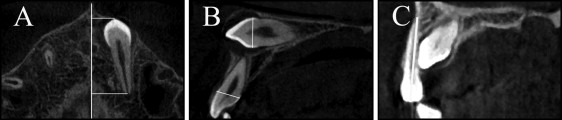
Fig 1 Cross-sectional CBCT images illustrating the reference lines of linear measurements: A, canine cusp tip and canine apex to the midline measured in the axial view; B, width of the canine and lateral incisor crown buccolingually measured in the sagittal view; C, length of the lateral incisor measured in the sagittal view. - 2.
Canine cusp tip to the occlusal plane was measured in the sagittal view. The occlusal plane was defined as the line from the mesiobuccal cusp of the maxillary first molar to the incisal edge of the maxillary central incisor in the sagittal view ( Fig 2 , A ).
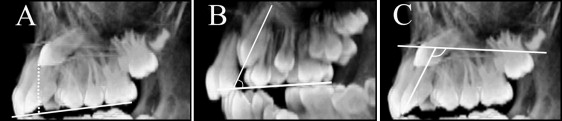
Fig 2 Cross-sectional CBCT images illustrating the reference lines of linear and angular measurements: A, canine cusp tip to the occlusal plane measured in the sagittal view; B, canine angulation to the occlusal plane measured in the sagittal view; C, lateral incisor inclination to the maxillary plane measured in the sagittal view. - 3.
Canine apex to the midline was measured in the axial view ( Fig 1 , A ).
- 4.
Width of the canine crown buccolingually and mesiodistally was defined as the distance from the mesial contour to the distal contour of the maxillary canine ( Fig 1 , B ).
- 5.
Width of the lateral incisor was measured buccolingually and mesiodistally at the cementoenamel junction ( Fig 1 , B ).
- 6.
Length of the lateral incisor from the incisal edge to the apex was measured in the sagittal view ( Fig 1 , C ).
- 7.
The mesiodistal space available for the canine between the lateral incisor and the first premolar at the occlusal level and at the apical thirds was measured in the axial view.
Angular measurements in degrees
- 1.
Canine angulation to the midline, where the angle is formed by the long axis of the impacted canine and the midline of the maxilla in the coronal view ( Fig 3 ).
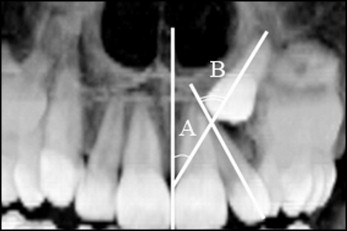
Fig 3 Coronal view of CBCT image illustrating the reference lines of the angular measurements: A , canine angulation to the midline; B , canine angulation to the lateral incisor. - 2.
Canine angulation to the lateral incisor, where an angle is formed by the long axis of the impacted canine and the long axis of the lateral incisor in the coronal view ( Fig 3 ).
- 3.
Canine angulation to the occlusal plane, where the angle in the sagittal view is formed by the long axis of the impacted canine and the occlusal plane ( Fig 2 , B ).
- 4.
Lateral incisor inclination to the maxillary plane, where the angle in the sagittal view is formed by the long axis of the lateral incisor and the maxillary plane ( Fig 2 , C ).
Statistical analysis
Analyses were performed on data from subjects with unilateral impaction. The aim of this study was to predict whether a canine would be impacted, not whether a patient had an impacted canine. Therefore, in the statistical analysis, independent instead of dependent tests were used; Fisher exact tests and Mann-Whitney U tests were used to compare scores and measurements between impacted and nonimpacted canines from patients with unilateral impaction. The area under the receiver operating curve (AUC) was reported for each score and measurement to quantify the discriminative ability (0.5 = random prediction, 1 = perfect discrimination). The reliability of the measurements was assessed using the records of 12 randomly selected patients and having the same investigator (A.A.) repeat the linear and angular measurements. The systematic error was evaluated with the intraclass correlation coefficient (ICC).
From these results, 6 variables were considered for a multivariable model, based on the AUC, clinical considerations, and the correlations among the variables. A backward selection procedure, with 0.157 as the critical level for the P value, was applied to obtain a more parsimonious prediction model. This critical value corresponds to the use of the Akaike information criterion (AIC) for model selection. With the AIC, we required the increase in the model’s chi-square value to be larger than 2 times the degrees of freedom. A bootstrap resampling procedure was used to verify whether the variables retained in the final multivariable model are truly independent predictors or, rather, are noise variables. In the applied modeling approach, the same data were used to develop and validate the model. Furthermore, there was a clear risk of overfitting, originating from consideration of many predictors compared with the number of impactions and from the application of an automated model selection procedure. The resulting prediction model and its related AUC were therefore overoptimistic, in the sense that the future performance in new patients was overestimated. Therefore, a leave-1-out cross-validation was applied. Also, an optimism-corrected estimate of the performance (AUC) was obtained by a bootstrap resampling procedure. All analyses were performed with SAS software (version 9.2 for Windows; SAS, Cary, NC).
Results
Tables I-III present comparisons of impacted and nonimpacted canines in terms of canine-related variables (scores), linear measurements, and angular measurements, respectively.
| Variable | Not impacted (%) | Impacted (%) | P value ∗ | AUC (95% CI) |
|---|---|---|---|---|
| Crowding | ||||
| No crowding | 75.3 | 76.9 | NS | 0.51 (0.43, 0.58) |
| Crowding | 24.7 | 23.1 | ||
| Deciduous canine | ||||
| Missing tooth | 78.5 | 52.3 | 0.007 | 0.64 (0.56, 0.72) |
| No resorption | 3 | 10.8 | ||
| Resorbed root | 18.5 | 36.9 | ||
| Canine development | ||||
| Complete development | 75.4 | 63 | NS | 0.56 (0.48, 0.64) |
| 3/4 of the root developed | 20 | 30.8 | ||
| 1/2 of the root developed | 4.6 | 6.2 | ||
| Open canine apex | ||||
| Closed or dilacerated | 41.5 | 29.2 | NS | 0.56 (0.48, 0.65) |
| Open | 58.5 | 70.8 | ||
| Abnormality | ||||
| No abnormality | 78.5 | 73.8 | NS | 0.52 (0.45, 0.60) |
| Abnormality | 21.5 | 26.2 | ||
| Rotation | ||||
| No rotation | 60 | 24.6 | <0.001 | 0.73 (0.65, 0.81) |
| Mesiovestibular rotation | 16.9 | 20 | ||
| Distovestibular rotation | 16.9 | 20 | ||
| Mesiopalatal rotation | 3.1 | 23.1 | ||
| Distopalatal rotation | 3.1 | 12.3 | ||
| Rotation | ||||
| No rotation | 60 | 24.6 | <0.001 | 0.68 (0.60, 0.76) |
| Rotation | 40 | 75.4 | ||
| Canine crown position | ||||
| Palatally | 4.6 | 47.7 | <0.001 | 0.85 (0.78, 0.91) |
| Buccally | 20 | 38.5 | ||
| Line of the arch | 75.4 | 13.8 | ||
| First premolar | ||||
| Single root | 21.5 | 18.5 | NS | 0.55 (0.46, 0.64) |
| Separated root | 52.3 | 46.1 | ||
| Two roots | 26.2 | 35.4 | ||
| Anterior apical area (axial) | ||||
| Optimal | 50.8 | 26.2 | 0.017 | 0.63 (0.54, 0.72) |
| Small | 32.3 | 47.7 | ||
| Severe | 16.9 | 26.1 | ||
| Contact relationship to lateral incisor | ||||
| No contact | 64.6 | 13.8 | <0.001 | 0.75 (0.68, 0.83) |
| Contact | 35.4 | 86.2 | ||
| Contact relationship to central incisor | ||||
| No contact | 100 | 83.1 | <0.001 | 0.59 (0.54, 0.63) |
| Contact | 0 | 16.9 | ||
| Contact relationship to first premolar | ||||
| No contact | 98.5 | 90.8 | NS | 0.54 (0.50, 0.58) |
| Contact | 1.5 | 9.2 | ||
∗ From Fisher’s exact or Mann-Whitney U test, as appropriate.
| Variable | Statistic | Not impacted | Impacted | P value ∗ | AUC (95% CI) |
|---|---|---|---|---|---|
| Canine cusp tip to midline | Mean (SD) | 14.7 (2.6) | 10.0 (4.2) | <0.001 | 0.86 (0.79, 0.93) |
| Median (range) | 15.2 (5.6-18.5) | 9.6 (0.0-24.0) | |||
| Canine cusp tip to occlusal plane | Mean (SD) | 3.6 (4.1) | 10.6 (4.3) | <0.001 | 0.88 (0.82, 0.94) |
| Median (range) | 2.7 (0.0-15.6) | 10.6 (0.0-22.5) | |||
| Canine apex to midline | Mean (SD) | 12.8 (1.7) | 13.9 (2.41) | 0.003 | 0.65 (0.56, 0.75) |
| Median (range) | 12.5 (9.3-17.0) | 13.8 (5.8-19.0) | |||
| Mesiodistal width of canine crown | Mean (SD) | 7.6 (0.5) | 7.8 (0.5) | NS | 0.60 (0.50, 0.69) |
| Median (range) | 7.6 (6.6-8.6) | 7.8 (6.7-8.9) | |||
| Buccolingual width of canine crown | Mean (SD) | 8.0 (0.6) | 8.1 (0.5) | NS | 0.55 (0.45, 0.65) |
| Median (range) | 7.9 (6.9-9.2) | 7.9 (7.4-9.2) | |||
| Mesiodistal width of the lateral incisor | Mean (SD) | 6.3 (0.7) | 6.4 (0.8) | NS | 0.57 (0.47, 0.67) |
| Median (range) | 6.3 (4.2-8.5) | 6.4 (3.9-9.1) | |||
| Buccolingual width of the lateral incisor | Mean (SD) | 6.4 (0.8) | 6.4 (0.6) | NS | 0.50 (0.50, 0.50) |
| Median (range) | 6.4 (3.1-7.9) | 6.4 (4.3-7.8) | |||
| Length of the lateral incisor | Mean (SD) | 21.8 (2.5) | 21.0 (3.2) | NS | 0.59 (0.49, 0.69) |
| Median (range) | 22.2 (13.6-26.7) | 21.4 (12.9-27.9) | |||
| Mesiodistal space at occlusal level | Mean (SD) | 7.0 (1.9) | 5.0 (2.9) | <0.001 | 0.74 (0.66, 0.83) |
| Median (range) | 7.4 (0.8-12.1) | 5.8 (0.0-11.4) | |||
| Mesiodistal space at apex level | Mean (SD) | 9.1 (1.9) | 8.0 (2.5) | 0.005 | 0.64 (0.55, 0.74) |
| Median (range) | 8.9 (3.2-13.2) | 7.6 (2.9-13.4) |
| Variable | Statistic | Not impacted | Impacted | P value ∗ | AUC (95% CI) |
|---|---|---|---|---|---|
| Canine angle to midline, coronal view | Mean (SD) | 8.8 (6.5) | 20.7 (14.9) | <0.001 | 0.77 (0.69, 0.85) |
| Median (range) | 6.9 (0.6-29.7) | 17.0 (1.1-62.7) | |||
| Canine angle to the lateral incisor, coronal view | Mean (SD) | 10.5 (8.5) | 36.3 (18.1) | <0.001 | 0.90 (0.85, 0.95) |
| Median (range) | 8.0 (1.2-38.9) | 38.0 (5.7-71.8) | |||
| Canine angle to the occlusal plane, sagittal view | Mean (SD) | 63.0 (12.52) | 52.9 (17.19) | <0.001 | 0.69 (0.59, 0.78) |
| Median (range) | 65.4 (18.7-86.3) | 54.6 (1.3-82.8) | |||
| Lateral incisor inclination to the maxillary plane, sagittal view | Mean (SD) | 106.4 (14.5) | 104.2 (18.9) | NS | 0.56 (0.45, 0.66) |
| Median (range) | 108.0 (11.8-126.9) | 105.8 (9.3-139.0) |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


