Radiation dose, dosimetry and dose limitation
Dose units
Radiation-absorbed dose (D)
| SI unit: | joules/kg (J/kg) |
| Special name: | Gray (Gy) |
| Subunit names: | milligray (mGy) (× 10−3) |
| microgray (µGy) (× 10−6) |
Equivalent dose (HT)
For example, alpha particles (see Ch. 18) penetrate only a few millimeters in tissue, lose all their energy and are totally absorbed, whereas X-rays penetrate much further, lose some of their energy and are only partially absorbed. The biological effect of a particular radiation-absorbed dose of alpha particles would be considerably more severe than a similar radiation-absorbed dose of X-rays.
| X-rays, gamma rays and beta particles | WR = 1 |
| Fast neutrons (10 keV – 100 keV) and protons | WR = 10 |
| Alpha particles | WR = 20 |
The equivalent dose (HT) in a particular tissue is therefore calculated as follows:Equivalent dose (HT) = radiation-absorbed dose (D) × radiation weighting factor (WR) in a particular tissue
| SI unit: | joules/kg (J/kg) |
| Special name: | Sievert (Sv) |
| Subunit names: | millisievert (mSv) (× 10−3) |
| microsievert (µSv) (× 10−6) |
For X-rays, the radiation weighting factor WR = 1, therefore the equivalent dose (HT) in a particular tissue, measured in Sieverts, is equal to the radiation-absorbed dose (D), measured in Grays.
Effective dose (E)
The tissue weighting factors recommended by the ICRP in 1990 and revised in 2007 are shown in Table 6.1.
Table 6.1
The tissue weighting factors (WT) recommended by the ICRP in 1990 and revised in 2007
| Tissue | 1990 WT | 2007 WT |
| Bone marrow | 0.12 | 0.12 |
| Breast | 0.05 | 0.12 |
| Colon | 0.12 | 0.12 |
| Lung | 0.12 | 0.12 |
| Stomach | 0.12 | 0.12 |
| Gonads | 0.20 | 0.08 |
| Bladder | 0.05 | 0.04 |
| Oesophagus | 0.05 | 0.05 |
| Liver | 0.05 | 0.04 |
| Thyroid | 0.05 | 0.04 |
| Bone surface | 0.01 | 0.01 |
| Brain | * | 0.01 |
| Kidneys | * | 0.01 |
| Salivary glands | – | 0.01 |
| Skin | 0.01 | 0.01 |
| Remainder tissues | 0.05* | 0.12† |
*Adrenals, brain, upper large intestine, small intestine, kidney, muscle, pancreas, spleen, thymus and uterus.
†Adrenals, extrathoracic airways, gallbladder, heart wall, kidney, lymphatic nodes, muscle, pancreas, oral mucosa, prostate, small intestine wall, spleen, thymus and uterus/cervix.
Effective dose (E) = ∑ Equivalent dose (HT) in each tissue × relevant tissue weighting factor (WT)
| Special name: | sievert (Sv) |
| Subunit names: | millisievert (mSv) (× 10−3) |
| microsievert (µSv) (× 10−6) |
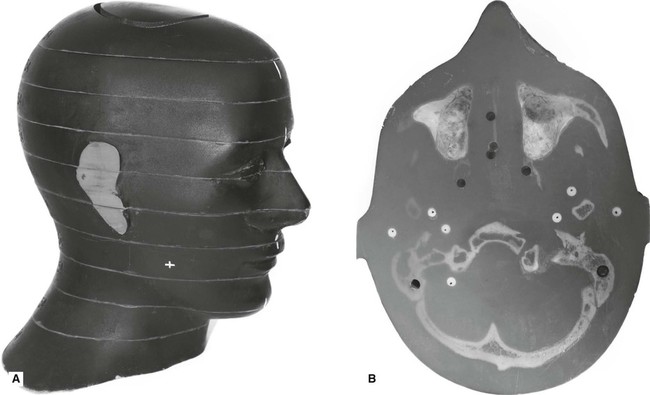
One way of calculating the effective dose is by using a tissue equivalent anthropomorphic phantom with dosimeters placed in the most radiosensitive regions, as shown in Fig. 6.1.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


