Differential diagnosis of radiolucent lesions of the jaws
Introduction
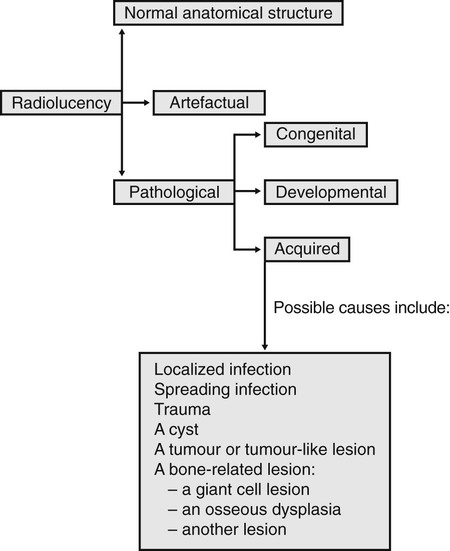
This chapter is designed to simplify the process of arriving at a radiological differential diagnosis when confronted with a radiolucency of unknown cause on a plain radiograph. This process requires clinicians to follow a methodical step-by-step approach and to know the typical features of the various possibilities. Such a step-by-step guide is suggested and summarized in Fig. 26.1. Although most lesions are still detected using plain radiographs, this process can be greatly facilitated in many cases if advanced imaging modalities, described in Chapters 16 and 18, such as computed tomography (CT), cone beam CT or magnetic resonance (MR), are available.
Step-by-step guide
Step IV
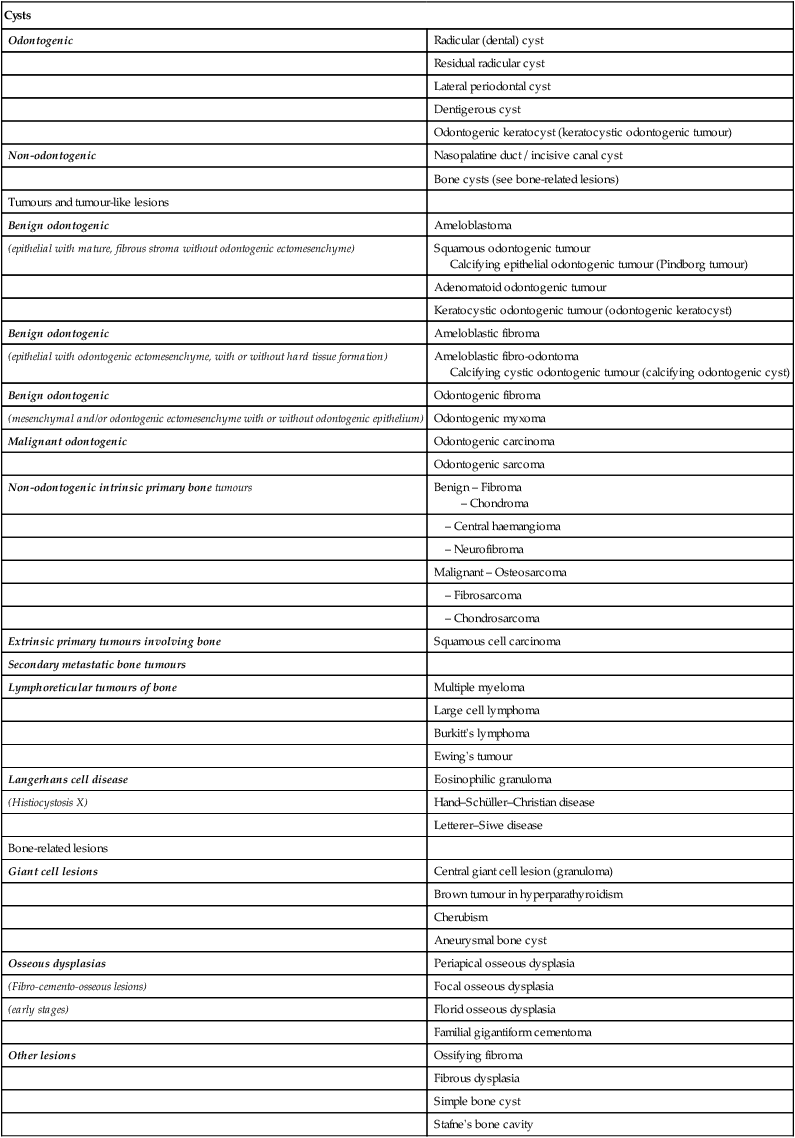
Consider the classification and subdivision of cysts and other similar radiolucencies within each of the other main disease categories, as shown in Table 26.1. This resultant list includes most of the more likely diagnostic possibilities for the unknown radiolucent lesion.
Table 26.1
| Cysts | |
| Odontogenic | Radicular (dental) cyst |
| Residual radicular cyst | |
| Lateral periodontal cyst | |
| Dentigerous cyst | |
| Odontogenic keratocyst (keratocystic odontogenic tumour) | |
| Non-odontogenic | Nasopalatine duct / incisive canal cyst |
| Bone cysts (see bone-related lesions) | |
| Tumours and tumour-like lesions | |
| Benign odontogenic | Ameloblastoma |
| (epithelial with mature, fibrous stroma without odontogenic ectomesenchyme) | Squamous odontogenic tumour Calcifying epithelial odontogenic tumour (Pindborg tumour) |
| Adenomatoid odontogenic tumour | |
| Keratocystic odontogenic tumour (odontogenic keratocyst) | |
| Benign odontogenic | Ameloblastic fibroma |
| (epithelial with odontogenic ectomesenchyme, with or without hard tissue formation) | Ameloblastic fibro-odontoma Calcifying cystic odontogenic tumour (calcifying odontogenic cyst) |
| Benign odontogenic | Odontogenic fibroma |
| (mesenchymal and/or odontogenic ectomesenchyme with or without odontogenic epithelium) | Odontogenic myxoma |
| Malignant odontogenic | Odontogenic carcinoma |
| Odontogenic sarcoma | |
| Non-odontogenic intrinsic primary bone tumours | Benign – Fibroma – Chondroma |
| – Central haemangioma | |
| – Neurofibroma | |
| Malignant – Osteosarcoma | |
| – Fibrosarcoma | |
| – Chondrosarcoma | |
| Extrinsic primary tumours involving bone | Squamous cell carcinoma |
| Secondary metastatic bone tumours | |
| Lymphoreticular tumours of bone | Multiple myeloma |
| Large cell lymphoma | |
| Burkitt’s lymphoma | |
| Ewing’s tumour | |
| Langerhans cell disease | Eosinophilic granuloma |
| (Histiocystosis X) | Hand–Schüller–Christian disease |
| Letterer–Siwe disease | |
| Bone-related lesions | |
| Giant cell lesions | Central giant cell lesion (granuloma) |
| Brown tumour in hyperparathyroidism | |
| Cherubism | |
| Aneurysmal bone cyst | |
| Osseous dysplasias | Periapical osseous dysplasia |
| (Fibro-cemento-osseous lesions) | Focal osseous dysplasia |
| (early stages) | Florid osseous dysplasia |
| Familial gigantiform cementoma | |
| Other lesions | Ossifying fibroma |
| Fibrous dysplasia | |
| Simple bone cyst | |
| Stafne’s bone cavity |
Step V
Infection is described elsewhere (apical, Ch. 21, spreading, Ch. 28) and trauma is described in Chapter 29. The rest of this chapter is devoted principally to differentiating between the different cysts – the most common of the remaining categories – and the other lesions that often present as very similar radiolucencies.
Typical radiographic features of cysts
Inflammatory odontogenic cysts
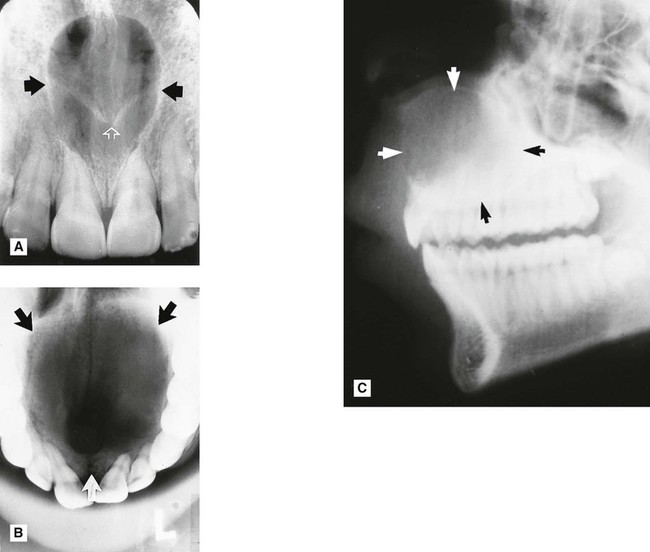
Radicular (dental) cyst (Fig. 26.2)
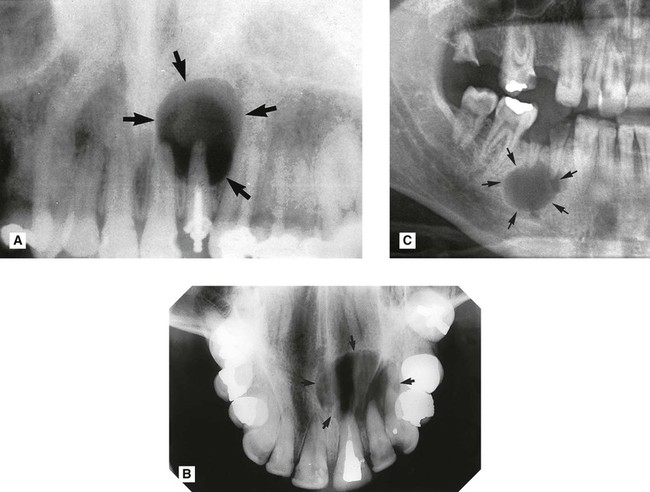
 . B Upper standard occlusal showing a large radicular cyst associated with the root-filled
. B Upper standard occlusal showing a large radicular cyst associated with the root-filled  . C Part of a panoramic radiograph showing a typical unilocular radicular cyst associated with the non-vital
. C Part of a panoramic radiograph showing a typical unilocular radicular cyst associated with the non-vital  .
.• Age: Usually adults, 20–50 year-olds.
• Frequency: Most common of all jaw cysts (about 70%).
• Site: Apex of any non-vital tooth, particularly upper lateral incisors.
• Size: 1.5–3 cm in diameter (if smaller the radiographic distinction between cyst and granuloma cannot usually be made).
— Well corticated if long-standing (unless infected) and continuous with the lamina dura of the associated tooth.
Note: The term buccal bifurcation cyst is used to describe an inflammatory odontogenic cyst that develops on the side of a molar tooth in relation to a buccal enamel spur or pearl.

Developmental odontogenic cysts
Lateral periodontal cyst (Fig. 26.4)

 and
and  . Although the adjacent premolar was restored, it was vital and symptom free.
. Although the adjacent premolar was restored, it was vital and symptom free.• Age: Adults over 30 years old.
• Site: Lateral surface of the roots of vital teeth in the lower canine/premolar region or upper lateral incisor region.
• Size: Small, less than 1 cm in diameter.
• Shape: —Unilocular, very occasionally multilocular
• Radiodensity: Uniformly radiolucent.
• Effects: —Adjacent teeth displaced if cyst becomes large, rarely resorbed
Dentigerous (follicular) cyst (Fig. 26.5)
This cyst develops from the remnants of the reduced enamel epithelium after the tooth has formed.
 />
/>
 . B Part of a panoramic radiograph showing a unilocular central dentigerous cyst (arrowed) associated with the unerupted and inferiorly displaced
. B Part of a panoramic radiograph showing a unilocular central dentigerous cyst (arrowed) associated with the unerupted and inferiorly displaced  . C Right side of a lower 90° occlusal of the same patient showing the typical buccal expansion (arrowed).
. C Right side of a lower 90° occlusal of the same patient showing the typical buccal expansion (arrowed).• Age: Usually adolescents or young adults, 20–40-year-olds, occasionally the elderly.
• Frequency: About 20% of all cysts.
• Site: Associated with the crown of an unerupted and displaced tooth, typically teeth where eruption is impeded, e.g.  and
and  .
.
• Size: Very variable, cyst suspected if follicular space exceeds 3 mm but may grow to several centimetres in diameter and extend up into the ramus.
• Shape: —Round or oval, typically enveloping the crown symmetrically
Note: The term eruption cyst is used to describe a dentigerous cyst when it is in the soft tissues overlying the unerupted tooth.
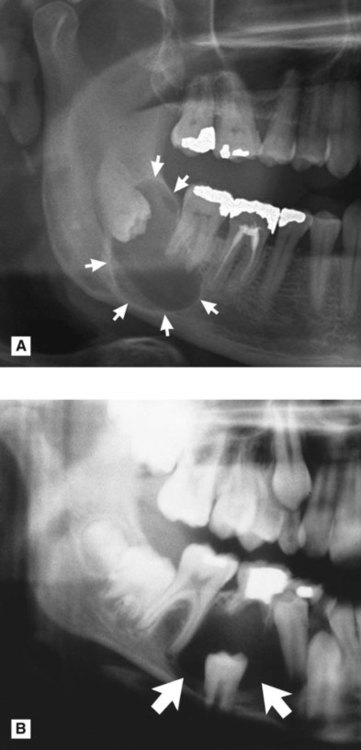
Odontogenic keratocyst (keratocystic odontogenic tumour) (Fig. 26.6)
 />
/> />
/>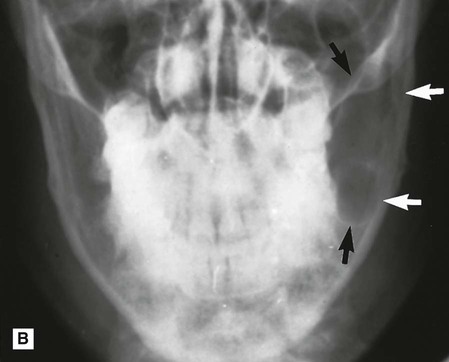
 . B PA jaws of the same patient showing that it has caused minimal mediolateral expansion (arrowed). C Left side of a panoramic radiograph showing a very large multilocular odontogenic keratocyst (arrowed) occupying almost all the left side of the mandible.
. B PA jaws of the same patient showing that it has caused minimal mediolateral expansion (arrowed). C Left side of a panoramic radiograph showing a very large multilocular odontogenic keratocyst (arrowed) occupying almost all the left side of the mandible.• Age: Very variable, peak incidence between second and third decades.
• Site: —Posterior body/angle of the mandible extending into the ramus
• Size: Variable, but often large in the mandible.
• Shape: —Oval, extending along the body of the mandible with little mediolateral expansion
• Outline: — Smooth and scalloped
• Radiodensity: Uniformly radiolucent.
• Effects: —Adjacent teeth – minimal displacement, rarely resorbed
 by enfolding so resembling a dentigerous cyst.
by enfolding so resembling a dentigerous cyst.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


