Introduction
Miniscrews often loosen during orthodontic treatment, especially in teenage patients. The purposes of this study were to explore the differences of the pullout strengths of miniscrews placed in the anterior mandibles of adolescent and adult dogs and the structural parameters of peri-miniscrew bone, and to analyze the correlation between the pullout strengths and the variables of the peri-miniscrew bone structure.
Methods
Eight adult beagles and 8 young beagles with early permanent dentitions were used as experimental subjects. Two miniscrews were symmetrically placed in the anterior mandible of each dog several minutes before death. The bone density, relative bone volume, and cortical bone thickness were evaluated by micro-computed tomography, and the pullout strength of the miniscrew was tested with a testing machine. Regression analyses were used to study the relationship between pullout strength and bone density, relative bone volume, and cortical bone thickness.
Results
The values of bone density, relative bone volume, cortical bone thickness, and pullout strength were 781.94 ± 21.46 mg of hydroxyapatite per cubic centimeter, 0.62 ± 0.33, 1.14 ± 0.11 mm, and 218.40 ± 24.50 N for the adult dogs; and 713.61 ± 13.08 mg of hydroxyapatite per cubic centimeter, 0.57 ± 0.20, 1.07 ± 0.86 mm, and 130.82 ± 2.20 N for the young dogs, respectively. All pairs of pullout force and bone structural parameters had significant correlation coefficients. The pullout force showed the strongest correlation with bone density and the weakest with cortical bone thickness.
Conclusions
The values of bone density, relative bone volume, cortical bone thickness, and the pullout strength of the adult group were higher than those of the young group. Furthermore, bone density is more sensitive in terms of showing pullout force compared with relative bone volume and cortical bone thickness.
Anchorage control is an important factor in successful orthodontic treatment. Various techniques have been devised and used in orthodontic practices to reinforce the anchorage. Miniscrews, originally used for intermaxillary or bone fixation, have been used as absolute anchorage during orthodontic treatment. With this skeletal anchorage, a wider range of tooth movements—intrusion, retraction, protraction, distalization, and uprighting—can be achieved without patient compliance. Compared with other temporary anchorage devices, miniscrews have the following advantages: minimal anatomic limitations for placement, lower medical costs, simpler placement and removal surgeries, less discomfort after placement, and immediate or early loading. The miniscrew has proven successful and is now useful in clinical applications. Although the reported success rate of the miniscrew is approximately 90%, in the clinic, miniscrews can loosen during orthodontic treatment, often in teenagers. Miyawaki et al found that the success rate of mini-implants in patients less than 20 years old (80%) was slightly lower than in those more than 20 years old (85%-88%). Park et al showed the importance of age for successful placement of mini-implants: implant failures were observed in 3 patients less than 14 years old, but there were no failures in 8 patients aged 14 to 28 years. Also, the success rate of miniscrews in patients under 16 years old was about 65% in a primary investigation (unpublished data). This is likely to be related to active bone metabolism and low maturation of the bone in growing patients. During childhood and adolescence, ossification occurs at a faster rate than bone resorption, so bones grow larger. During the early and middle years of adulthood, bones neither grow nor shrink, but, after the age of 35 to 40 years, bone loss exceeds bone gain.
When a mechanical evaluation of the stability of screw-shaped implantation including miniscrews is made, placement and removal torques and pullout strengths used to evaluate the shear strength of the bone-implant interface are generally measured. An and Draughn showed that the experimental setup of a torque test is more elaborate than that required for a pullout test. A pullout test is widely used because of the relative simplicity of its protocol, which usually requires a uniaxial materials testing machine operated under displacement control with a simple support jig for the push-out test or a hookup system for the pullout test. Although more reports have shown that these immediately or early loaded miniscrews can provide good anchorage control, the stability of miniscrews in teenagers and young animals has seldom been reported. The purposes of this study were to record the pullout strengths of miniscrews placed in the anterior mandibles of adult and adolescent dogs, analyze the peri-miniscrew bone structure by using microcomputed tomography (μCT), and explore the correlation between the pullout strengths and the variables of peri-miniscrew bone structure.
Material and methods
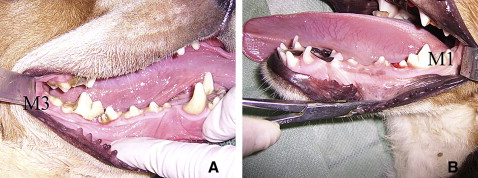
Sixteen male beagles were used as experimental subjects. They were divided into 2 groups according to age and dental age; each group had 8 beagles. The adult dogs were 23 to 24 months old and weighed 13 to 14 kg; their mandibular third molars had erupted ( Fig 1 , A ). The dogs in young group were about 9 months old and weighed 8 to 8.5 kg; their mandibular second and third molars had not erupted ( Fig 1 , B ). The experiment was approved by the bioethics committee of Sichuan University, Chengdu, China. The veterinary records indicated that the dogs were healthy.
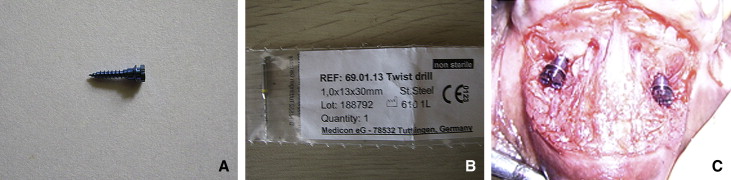
Thirty-two Aarhus miniscrews (diameter, 1.6 mm; length, 6 mm) provided by the manufacturer (Medicon, Tuttlingen, Germany) were placed in anterior regions of the mandibles ( Fig 2 , A ). Each dog received 2 miniscrews several minutes before death. The 2 miniscrews placed in each dog were placed on the left and right sides symmetrically. The surgical implant procedure was as follows. A mucoperiosteal flap between the 2 mandibular canines was opened, and the alveolar bone was denuded. The cortical bone was drilled with a 1.0-mm pilot drill ( Fig 2 , B ) with water cooling for the length of the cortical bone thickness. The miniscrew was placed with a miniature screwdriver to the screw neck; we intended to place the screw perpendicular to the cortical bone surface ( Fig 2 , C ).
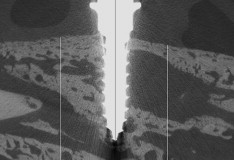
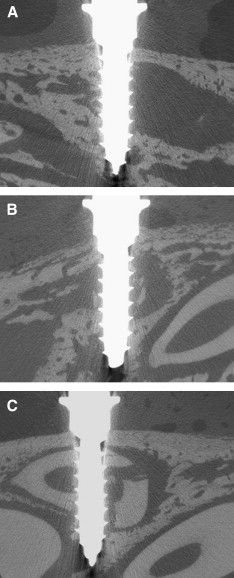
When the dogs were killed, their jaws were removed and sectioned into small blocks within 30 minutes, each containing 1 screw, which was surrounded by at least 4 mm of tissue with no soft tissue ( Fig 3 , A ). The blocks were transferred to phosphate-buffered formalin for 48 hours and kept in 70% ethanol. For a detailed qualitative and quantitative 3-dimensional (3D) evaluation, the proximal 4 mm of bone around the miniscrew was examined with an imaging system (μCT 80, Scanco Medical, Bassersdorf, Switzerland). For image acquisition, the specimens were mounted on a turntable shifted automatically in an axial direction vertical to the long axis of the miniscrew. The x-ray tube voltage was set to 70 kV to allow maximum x-ray transmission through the highly opaque titanium implant. To maximize the signal-to-noise ratio, the system was operated at 114 mA (maximum current for the 70-kV setting) and the longest integration time (300 ms). The distance between 2 adjacent slices was 20 μm. The titanium and cortical bone were segmented from each other and from trabecular bone with a multi-level thresholding procedure. The peri-miniscrew bone region of interest included the entire bone compartment between the cross-sectional planes 2.8 mm proximally and 2.8 mm distally from the miniscrew longitudinal axis ( Fig 4 ). In the analyses of bone specimens, 140 consecutive slices were reconstructed, excluding the teeth and the miniscrew; 3D bone morphometric quantitative data were calculated to explore micro-structural specifications of bone near the screw. The parameters obtained with μCT included: bone density (milligrams of hydroxyapatite per cubic centimeter [mg HA/cm 3 ]) of total volume (TV) and relative bone volume (BV/TV). In the middle slice of the miniscrew ( Fig 5 , A and B ), we measured cortical bone thickness.
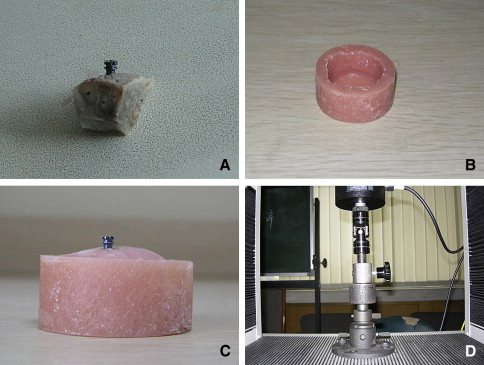
After the μCT analysis, the specimens were progressively rehydrated and kept in phosphate-buffered saline solution for 48 hours before the biomechanical testing. For pullout testing, the screw must be aligned with the axis of the testing machine. This ensured that no bending moment was created during the pullout test and that only axial pullout strengths were recorded. So, a custon-made cylinder of acrylic resin with a hole was designed ( Fig 3 , B ). The bone-screw block was embedded in the hole with acrylic resin. The specimen was about 2 mm higher than the upper plane of the cylinder so that it was easy to clamp the screw head to the jig. The screw was placed in the center of the cylinder, and the long axis of the screw was vertical to the plane of the cylinder ( Fig 3 , C ). Determination of the pullout strength is a standardized method of testing the mechanical competency or holding power of a screw. To observe the effects of test variables, standardized biomechanical tests must be conducted. The testing machine used for the pullout test is shown in Figure 3 , D (AG-IS stretching machine, Trapezium Soft, Shimadzu, Japan). The cylinder including the bone-screw block was fixed on the base of the machine. The head of the miniscrew was clamped by a universal jig designed specifically for this study that could be adjusted in all directions. To avoid prestress, we corrected the system after fixing the bone-screw block and clamping the screw head. A crosshead speed of 2 mm per minute was applied to extract the screw. The load-displacement data were recorded, and the peak load at failure was obtained from the data file.
Pullout force, bone density, BV/TV, and cortical bone thickness of the adult and young dogs were analyzed by using t tests. The results were considered significant at P <0.05. Regression analyses were used to study the relationship between pullout strength (dependent variable) and bone density, BV/TV, and cortical bone thickness (independent variable). These analyses were carried out with statistical analysis software (version 12.0, SPSS, Chicago, Ill).
Results
Twenty-two miniscrews were placed in the mandibular anterior regions; μCT examination of the bone-screw blocks showed that 3 miniscrews were placed through the roots of adjacent teeth ( Fig 5 , C ), 1 in the left mandible of an adult dog, and the others in the left or right mandible of 2 young dogs; the other miniscrews were placed in bones. Although all miniscrews were tested by the pullout method, we analyzed only the 29 blocks with the screws in the bones.
The values of the bone density were 781.94 ± 21.46 mg of HA per square centimeter for the adult dogs and 713.61 ± 13.08 mg of HA per square centimeter for the young dogs ( Table I ). There were statistically significant differences in bone density between the groups of dogs ( P = 0.000).
| Group | n | Maximum | Minimum | Mean | SD | P |
|---|---|---|---|---|---|---|
| Adult dogs | 15 | 823.98 | 758.36 | 781.94 | 21.46 | 0.000 |
| Young dogs | 14 | 738.94 | 698.37 | 713.61 | 13.08 |
The values of BV/TV were 0.62 ± 0.33 for the adult dogs and 0.57 ± 0.20 for the young dogs ( Table II ). There were statistically significant differences in BV/TV between the groups ( P = 0.000).
| Group | n | Maximum | Minimum | Mean | SD | P |
|---|---|---|---|---|---|---|
| Adult dogs | 15 | 0.69 | 0.58 | 0.62 | 0.33 | 0.000 |
| Young dogs | 14 | 0.60 | 0.54 | 0.57 | 0.20 |
The cortical bone thicknesses were 1.14 ± 0.11 mm for the adult dogs and 1.07 ± 0.86 mm for the young dogs ( Table III ). There were no significant differences in cortical bone thickness between the groups ( P = 0.060).
| Group | n | Maximum | Minimum | Mean | SD | P |
|---|---|---|---|---|---|---|
| Adult dogs | 15 | 1.34 | 0.98 | 1.14 | 0.11 | 0.060 |
| Young dogs | 14 | 1.16 | 0.89 | 1.07 | 0.86 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


