Fig. 6.1
Normal periodontal tissues
The oral mucosa is the tissue lining the oral cavity [5] and is termed by its specific anatomical location. For example, the alveolar mucosa is the loosely attached and movable mucosa covering the basal part of the alveolar process and continuing into the vestibular fornix and the floor of the mouth [5, 12].
The gingiva is the fibrous investing tissue that surrounds a tooth and is contiguous with its periodontal ligament and with the mucosal tissues of the mouth [5]. The gingiva is divided into free gingiva and attached gingiva and is considered as a part of the masticatory mucosa, which covers the alveolar process and surrounds the cervical portion of the teeth. It consists of an epithelial layer and an underlying connective tissue layer. The gingiva obtains its final form and texture with the eruption of the teeth [13].
The attached gingiva is the portion of the gingiva that is firm, dense, stippled, and firmly bound to the underlying periosteum, tooth, and bone [5]. The width of the attached gingiva varies in range from 1 to 9 mm in different parts of the mouth [14]. In the maxilla, the facial attached gingiva is generally widest in incisors and most narrow adjacent to the canine and first premolars. In the mandible, the gingiva on the lingual aspect is particularly narrow in the area of the incisors and canines and widest in the molar region [15]. Facially positioned teeth had narrower zones of attached gingiva compared to well-aligned or lingual positioned teeth [16].
The free gingiva is the part of the gingiva that surrounds the tooth and is not directly attached to the tooth surface [5]. The free gingival margin is the coronal part of the gingiva and has a scalloped outline. The free gingival margin is situated about 2 mm coronal to the CEJ of the tooth, and the attached gingiva extends from the base of the free gingiva to the mucogingival junction [5, 9, 12].
The gingiva is continuous with the alveolar mucosa that is situated apically. The mucogingival junction is the demarcated border between the gingival and the alveolar mucosa and is absent in the palatal aspect of the maxillary teeth where the gingiva is continuous with the palatal mucosa [5, 12]. The mucogingival junction defines the width of the attached gingiva.
The gingival papilla is the portion of the gingiva that occupies the interproximal spaces [5]. The shape of the papilla is influenced by the shape of the interproximal contact points, the width of the interproximal area, and the position of the CEJ of the involved teeth, and it may vary from triangular and knife-edge shapes in the anterior regions to a more square shaped in the posterior regions [5, 12].
The gingival sulcus is a fissure that is an invagination around a tooth bounded by the free gingival margin [5, 12] and ranges between 0 and 6 mm depth (average depth of 0.7 mm) [12]. The alveolar bone follows a path that parallels the positions of the CEJs of the teeth, and in health the interdental bone is about 1 mm from the CEJ and increases with age to about 3 mm [12].
The supracrestal connective tissue attachment is the connective tissue fibers that originate from the osseous crest to the CEJ; the epithelial attachment (or junctional epithelium) is the epithelial attachment from the CEJ onto the tooth enamel.
The Etiology and the Possible Risk Factors of Flap-Related Complications
Flap procedures may lead to several complications [4, 6–8, 10, 12, 17], including attachment loss and recession of the gingival margin, flap necrosis, flap tearing, tissue dehiscence, delayed healing, periodontal defect, scarring, hemorrhage, and nerve injury.
Following endodontic surgery, and consistent with the basic biological principles of wound healing, the postsurgical histological wound healing sequel can be repair (when the injured tissues are replaced with scar tissue) or regeneration (when the injured tissues are reestablished by similar tissue as was originally present) [18].
Clinically, the soft tissue healing can be divided to healing by first intention, e.g., primary union of a wound in which the incised tissue edges are approximated and held until union occurs, and to healing by second intention, e.g., wound closure wherein the edges remain separated and the wound heals from the base and sides via the formation of granulation tissue [5]. In wounds healing by second intention, continuous local inflammation, infection, wound dehiscence, and foreign bodies are important contributory factors to an ensuing scar formation [19].
Scarring: A scar can be defined as fibrous tissue replacing normal tissues destroyed by injury or disease [5]. Macroscopically a scar is a disturbance of the normal structure and function of the tissue architecture, resulting from the end product of the healed wound [10]. Histologically, scars are characterized by their lack of specific organization of cellular and matrix elements when compared with the uninjured tissue [19]. The normal wound healing process includes a combination of biological processes such as hemostasis, inflammation, proliferation, and remodeling. Scar formation may occur as a result of altered regulation of the normal physiological processes in the involved epithelial and submucosal tissues. The scarring may clinically manifest as an elevated or depressed site, with an alteration of the mucosal texture and color and changes in the biomechanical properties of the tissues [4]. From a clinical point of view, scar formation following flap procedure is a significant esthetic problem, especially in the esthetic zone and in patients with a high smile line (i.e., a significant exposure of maxillary anterior gingiva during a full smile) [20] (Fig. 6.2).

Fig. 6.2
Scar following submarginal incision
Attachment loss refers to the distance between the CEJ and the base of the gingival sulcus and may manifest both as probing pocket depth and\or gingival recession.
Gingival recession is the location of marginal periodontal tissues apical to the CEJ that may be caused by improper periodontal surgical manipulations [4, 6–8, 10, 12, 17], such as incorrect reposition of the flap, compromised blood circulation of the flap through excessive retraction or poor flap design, and flap contraction [4, 7, 8, 10–12, 19, 21] (Fig. 6.3). Thus, it is important to preserve the root-attached tissues and to reposition a tension-free flap.

Fig. 6.3
Gingival recession
Flap necrosis may occur because of insufficient blood supply. The prevention of flap necrosis includes vertical releasing incisions that should be parallel or converging to the coronal part of the flap; the base of the flap should be wider than the free margin to allow an adequate blood supply, and it is advised to avoid excessive force or crashing of the tissue with the retractors [1, 7].
Flap tearing may occur as a result of poor flap design with a small and insufficient incision that causes flap tension and may result in tearing (Fig. 6.4). Thus, the flap should be reflected as one unit, with sufficient length of releasing incisions [1, 7]. It should be remembered that the flap incision wound naturally heals from side to side and not end to end. Thus, a long incision does not necessarily heal slower.

Fig. 6.4
Flap tear following endodontic surgery on the mandibular incisors
Soft tissue dehiscence is usually a result of infection from bacterial contamination of the incisional wound. Partial or total separation of the wound margins may manifest within the first week after surgery. In most instances, the wound dehiscence results from tissue failure rather than improper suturing techniques. The dehisced wound may be closed again or left to heal by secondary intention, depending upon the extent of the disruption and the surgeon’s judgment of the clinical situation [22].
Influence of a Periodontal Disease on Soft Tissue Healing Following Endodontic Surgery
Periodontal diseases are infections and are caused by microorganisms that colonize the tooth surface at the gingival margin. Sometimes, a combination of factors (e.g., bacteriological or treatment-related factors) facilitates conditions that may promote either a colonization of newly introduced subset of bacterial species or an overgrowth of existing bacterial species that may eventually lead to a destruction of the periodontium [13].
It has been reported that when performing modern endodontic surgery for teeth with endodontic-periodontal combined lesions, the endodontic success rate is expected to drop to less than 80 %, compared to 95 % for cases with an isolated endodontic lesions [23]. In addition, preoperative factors significant for the prognosis of restored endodontically treated teeth are related to the periodontal status and the attachment loss [24]. Thus, the presence of a significant periodontal disease may adversely affect the success of the endodontic surgery [23], the expected long-term survival of the tooth [24], and the risk and extent of flap-related complications.
The Gingival Biotype Effects on the Surgical Procedure
Recently, it was demonstrated that the gingival biotype could be related to complications following flap procedures [8, 11].
There are two distinctive types of gingival phenotypes: thick and thin gingival biotypes.
Thin gingival biotype is more prevalent in women and is characterized by a highly scalloped marginal gingiva with slender teeth, with delicate and almost translucent appearance, and with a minimal narrow zone of attached gingiva [7, 11, 17].
Thick gingival biotype is more prevalent in men and is characterized with a bulky, slightly scalloped marginal gingiva with short and wide teeth, broad zone of attached gingiva, fibrotic and resilient tissue, relatively flat soft tissue, and a relatively large amount of attached gingiva [7, 11, 17].
Several methods were proposed based on the measurement of buccal gingival thickness to assess gingival biotypes, and the simplest method is based on using the transparency of a periodontal probe through the gingival margin. If the outline of the probe could be visually detected through the tissue, it should be categorized as thin biotype; if not, it should be categorized as a thick biotype [8, 11, 25] (Fig. 6.5). Several periodontal and anatomical parameters were suggested to be associated with a specific gingival biotype, such as the tooth shape and contact point location, papilla height, and the distance from the contact point to the alveolar crest. Additional demographic factors, such as the patient age, may also be associated [11].
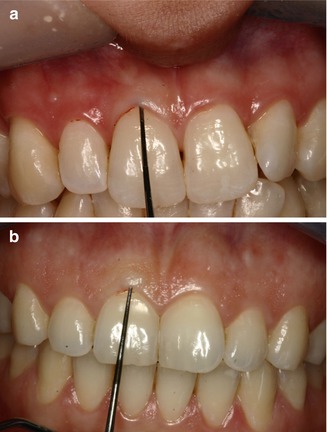
Fig. 6.5
Gingival biotypes assessment. (a) thin periodontal biotype, (b) thick periodontal biotype
The identification of the gingival biotype is important in planning the type of surgical incision during endodontic surgery, since various gingival biotypes may influence the esthetic outcome of surgery [17]. It may be especially crucial in the esthetic area, since thin gingival biotypes may be a risk factor of postsurgical recession development [8, 11].
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


