Introduction
The aim of this study was to compare the pattern and prevalence of associated dental anomalies between maxillary and mandibular tooth agenesis (hypodontia).
Methods
A sample of 3315 dental patients, aged 8.6 to 25.4 years, was surveyed for tooth agenesis (excluding third molars): 106 subjects were diagnosed with maxillary hypodontia (group 1) and 70 with mandibular hypodontia (group 2). Both groups were examined for the following dental anomalies: retained deciduous molars, infraocclusion of deciduous molars, impaction, microdontia of maxillary lateral incisors, supernumerary teeth, transposition, transmigration, and ectopic eruption of the permanent molars. For statistical testing, the chi-square test ( P <0.05) was used to compare the occurrences of these anomalies among the groups.
Results
We found that 77.5% of the patients in the mandibular hypodontia group had at least 1 dental anomaly compared with 49.5% in the maxillary hypodontia group ( P <0.0001). The only dental anomaly with a significantly increased prevalence in the maxillary hypodontia group compared with the mandibular hypodontia group was microdontia of the maxillary lateral incisors (groups 1, 46.7%; group 2, 12.9%; P <0.0001). On the other hand, the prevalences of retained deciduous molars (group 1, 9.4%; group 2, 60.0%), infraoccluded deciduous molars (group 1, 0.9%; group 2, 7.1%), and impacted teeth (group 1, 22.6%; group 2, 38.6%) were significantly higher in the mandibular hypodontia group. The prevalences of supernumerary teeth, transposition, transmigration, and ectopic eruption of permanent molars were low and not significantly different between the groups.
Conclusions
Tooth agenesis isolated to the maxilla is frequently associated with microdontia of the maxillary lateral incisors, whereas tooth agenesis isolated to the mandible is frequently associated with retained deciduous molars, infraoccluded deciduous molars, and impacted teeth. The results of this study may provide additional evidence supporting the field-specific genetic control theory for dental development in both jaws.
Highlights
- •
Maxillary tooth agenesis is associated with maxillary lateral incisor microdontia.
- •
Mandibular tooth agenesis is associated with multiple anomalies.
- •
Dental development in both jaws may be under field-specific genetic control.
- •
Diagnosing one dental anomaly should alert the clinician to the risk of others.
Tooth agenesis, also known as hypodontia, is a common dental anomaly, with reported incidences of 2.7% to 12.2% in the permanent dentition (excluding third molars). This anomaly is not usually an isolated phenomenon; it is frequently reported with other dental anomalies such as peg-shaped lateral incisors, transposition, impaction, delayed dental development, ectopic eruption, retained deciduous teeth, and other abnormalities in the size and shape of teeth. The concurrence of these anomalies along with hypodontia in the same patient may suggest that these different dental phenotypic expressions are a result of the same genetic mutation. Therefore, extensive research was conducted to determine the genetic basis for this anomaly, and mutations in a number of genes were identified. Different models of inheritance for this anomaly have also been suggested, including autosomal dominant with incomplete penetrance, autosomal recessive, sex-linked inheritance, and polygenic model of inheritance.
Previous studies have reported the association of specific tooth agenesis with different dental anomalies and compared the results with a nonhypodontia control group or with the reported incidence of these anomalies in the general population. In this study, on the other hand, we aimed to investigate whether the prevalence and pattern of the dental anomalies associated with hypodontia isolated in the maxilla were different from those isolated in the mandible. This investigation may provide further evidence on field-specific genetic control of dental development. The null hypothesis was that the specific site of hypodontia does not predict the prevalence and distribution of associated dental anomalies.
Material and methods
The study sample included patients who attended the orthodontic and pediatric departments of the dental school at the University of Jordan in Amman between 2011 and 2014. Patients with incomplete records, previous history of orthodontic treatment, or craniofacial syndromes and clefts were excluded. A total of 3315 records (34.3% male, 65.7% female) for dental patients aged 8.6 to 25.4 years (mean age, 17.3 years; SD, 4.7 years) were surveyed by 2 calibrated examiners (M.A., A.A.) concurrently. The main examined records were digital orthopantomograms, and the investigators had access to photographs, intraoral radiographs, and study models on request.
Odontogenesis and onset of mineralization of the mandibular second premolars were reported to show great variability. Nevertheless, the lower limit of the age of our sample was convenient to study hypodontia of all permanent teeth (excluding third molars) with minimal false-positive findings. Tooth agenesis was diagnosed when there was no sign of crown calcification on the radiograph and no evidence or history of loss attributable to orthodontic treatment, caries, periodontal disease, or trauma. Patients with tooth agenesis affecting both arches were excluded, and the remaining subjects were divided into 2 groups: group 1 (agenesis in the maxillary arch only) and group 2 (agenesis in the mandibular arch only).
The dental anomalies investigated in this study were the following.
- 1.
Retained deciduous molars: deciduous molars maintained in the arch with missing permanent successors.
- 2.
Impaction: a tooth that is predicted to remain unerupted because of a physical barrier or deflection along its eruption path. A maxillary canine that is impacted and displaced palatally was termed a palatally displaced canine (PDC). The radiographic parameters described by Lindauer et al were used to diagnose impaction, and intraoral radiographs were examined to confirm the position of the impacted canine.
- 3.
Microdontia of the maxillary lateral incisors: when the mesiodistal width of the crown is less than that of the opposing mandibular lateral incisor.
- 4.
Infraocclusion of the deciduous molars: when the retained deciduous molar (with no permanent successor) is at or below the contact point of the adjacent teeth.
- 5.
Transposition: exchanged positions of 2 adjacent teeth in the same quadrant.
- 6.
Supernumerary teeth: teeth that appear in addition to the regular number of teeth.
- 7.
Transmigration: when an impacted tooth crosses the midline regardless of the distance.
- 8.
Ectopic eruption of permanent molars: eruption in an abnormal position.
Statistical analysis
SPSS software (version 19.0; IBM, Armonk, NY) was used for the statistical analysis. Subjects in the maxillary hypodontia group and the mandibular hypodontia group were compared for age and number of missing teeth using the independent sample t test and for sex distribution using the chi-square test. Descriptive statistics and frequency tables were then created for general descriptions of the results in both groups. The prevalences of associated dental anomalies in each group were compared with the chi-square test. The level of significance was set at P <0.05.
Results
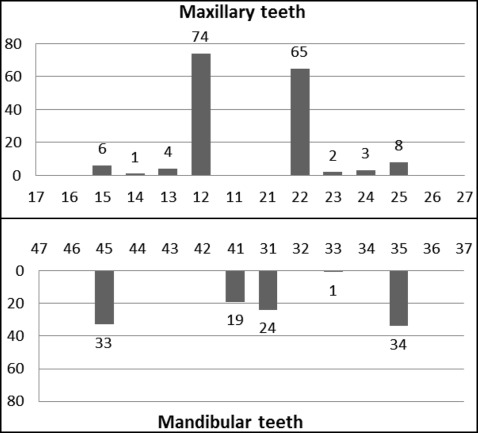
At least 1 missing permanent tooth was identified in 217 patients (39.2% in males, 60.8% in females) from the total sample of 3315 patients. Agenesis diagnosed in both arches accounted for 18.9% (n = 41), and these subjects were excluded. Maxillary hypodontia was seen in 106 patients (group 1), and mandibular hypodontia was seen in 70 patients (group 2), with no significant difference in the sex distribution between the groups (χ 2 = 0.38; P = 0.54). Table I compares the ages and numbers of missing teeth between the maxillary hypodontia group and the mandibular hypodontia group. The mean ages were 17.1 years in the maxillary hypodontia group and 15.9 years in the mandibular hypodontia group, with no significant difference ( P = 0.051). The total number of missing teeth, excluding third molars, was 274 with an average of 1.6 teeth per patient (minimum, 1; maximum, 4). The numbers of missing teeth were not significantly different between the groups, and the distribution of individual missing teeth is shown in Figure 1 . In the maxillary arch the most frequent missing teeth were the lateral incisors (87.7%), followed by the second premolars (10.4%). In the mandibular arch the most common missing teeth were the second premolars (64.3%), followed by the central incisors (38.6%).
| Group | Range | Mean | SD | t test value | P value | 95% Confidence limits | |
|---|---|---|---|---|---|---|---|
| Age (y) | 1 | 8.6-25.4 | 17.1 | 4.5 | 2.0 | 0.051 | −0.01 to 2.9 |
| 2 | 8.6-24.9 | 15.9 | 4.6 | ||||
| Missing teeth (n) | 1 | 1-4 | 1.6 | 0.6 | 0.34 | 0.73 | −0.16 to 0.2 |
| 2 | 1-4 | 1.5 | 0.6 |
The prevalence of dental anomalies in the mandibular hypodontia group (77.5%) was significantly higher than in the maxillary hypodontia group (49.5%), with a chi-square value of 13.9 and P <0.0001. When the number of dental anomalies in subjects with 1 missing tooth from both groups was compared with those with 4 missing teeth, there was no significant difference ( t test value, −0.22; P = 0.65; 95% confidence limits, −1.24 to 0.99). Therefore, there was no association between the severity of hypodontia and the number of dental anomalies.
The distributions of dental anomalies between the maxillary hypodontia group and the mandibular hypodontia group, as well as the chi-square test results, are shown in Table II . After excluding subjects with bilateral agenesis of maxillary lateral incisors (n = 46) from the maxillary hypodontia group (n = 106), it was found that the most commonly prevalent dental anomaly in the maxillary hypodontia group was microdontia of the maxillary lateral incisor (46.7%), and it was the only dental anomaly in the maxillary hypodontia group that was significantly higher than in the mandibular hypodontia group (χ 2 = 18.1; P <0.0001). On the other hand, there were 3 dental anomalies in the mandibular hypodontia group that were significantly higher than in the maxillary hypodontia group: retained deciduous molars (group 1, 9.4%; group 2, 60.0%), infraoccluded deciduous molars (group 1, 0.9%; group 2, 7.1%), and impacted teeth (group 1, 22.6%; group 2, 38.6%).
| Dental anomaly | Group 1, n = 106 | Group 2, n = 70 | χ 2 | P |
|---|---|---|---|---|
| Retained E | 10 (9.4%) | 42 (60.0%) | 48.1 | <0.0001 ∗ |
| Impaction | 24 (22.6%) | 27 (38.6%) | 5.2 | 0.023 ∗ |
| PDC | 10 (9.4%) | 10 (14.3%) | 1.2 | 0.27 |
| Small maxillary lateral incisors | 28 † (46.7%) | 9 ‡ (12.9%) | 18.1 | <0.0001 ∗ |
| Infraocclusion E | 1 (0.9%) | 5 (7.1%) | 4.9 | 0.027 ∗ |
| Transposition | 5 (4.7%) | 1 (1.4%) | 1.4 | 0.24 |
| Supernumerary teeth | 3 (2.8%) | 2 (2.9%) | <0.001 | 0.99 |
| Transmigration | 1 (0.9%) | 2 (2.9%) | 0.9 | 0.34 |
| Ectopic eruption of 6 | 0 | 0 | – | – |
| Ectopic eruption of 7 | 1 (0.9%) | 0 | – | – |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


