Introduction
Digital impression devices are used alternatively to conventional impression techniques and materials. The aims of this study were to evaluate the precision of digital intraoral scanning under clinical conditions (iTero; Align Technologies, San Jose, Calif) and to compare it with the precision of extraoral digitization.
Methods
One patient received 10 full-arch intraoral scans with the iTero and conventional impressions with a polyether impression material (Impregum Penta; 3M ESPE, Seefeld, Germany). Stone cast models manufactured from the impressions were digitized 10 times with an extraoral scanner (D250; 3Shape, Copenhagen, Denmark) and 10 times with the iTero. Virtual models provided by each method were roughly aligned, and the model edges were trimmed with cutting planes to create common borders (Rapidform XOR; Inus Technologies, Seoul, Korea). A second model alignment was then performed along the closest distances of the surfaces (Artec Studio software; Artec Group, Luxembourg, Luxembourg). To assess precision, deviations between corresponding models were compared. Repeated intraoral scanning was evaluated in group 1, repeated extraoral model scanning with the iTero was assessed in group 2, and repeated model scanning with the D250 was assessed in group 3. Deviations between models were measured and expressed as maximums, means, medians, and root mean square errors for quantitative analysis. Color-coded displays of the deviations allowed qualitative visualization of the deviations.
Results
The greatest deviations and therefore the lowest precision were in group 1, with mean deviations of 50 μm, median deviations of 37 μm, and root mean square errors of 73 μm. Group 2 showed a higher precision, with mean deviations of 25 μm, median deviations of 18 μm, and root mean square errors of 51 μm. Scanning with the D250 had the highest precision, with mean deviations of 10 μm, median deviations of 5 μm, and root mean square errors of 20 μm. Intraoral and extraoral scanning with the iTero resulted in deviations at the facial surfaces of the anterior teeth and the buccal molar surfaces.
Conclusions
Scanning with the iTero is less accurate than scanning with the D250. Intraoral scanning with the iTero is less accurate than model scanning with the iTero, suggesting that the intraoral conditions (saliva, limited spacing) contribute to the inaccuracy of a scan. For treatment planning and manufacturing of tooth-supported appliances, virtual models created with the iTero can be used. An extended scanning protocol could improve the scanning results in some regions.
For the introduction of computer-aided design and computer-aided manufacturing technologies in dentistry, virtual models of teeth are required. Digital processes are applied for prosthetic-driven backward planning of implant surgery, orthodontic measurements, and treatment planning combined with surgical planning. Data acquired by intraoral scanning, computed tomography, cone-beam computed tomography, and extraoral surface scanning can be fused.
For the acquisition of digital images of teeth, different procedures have been described: digitization of plaster casts, digitization of impressions, and intraoral digital impressions. The accuracy of the different image acquisition methods and systems has been examined with extraoral reference models. However, to date, no studies concerning the practical application and precision of digital scanning in vivo have been done.
Digital work flow has been proposed to improve treatment planning, give higher efficiency, and allow new methods of production and new treatment concepts. Data storage and reproducibility are facilitated, and treatment documentation and communication between professionals as well as between dentists and patients have become more convenient.
Currently, there are a few major digital impression devices: iTero (Align Technologies, San Jose, Calif), Lava COS (3M ESPE, Seefeld, Germany), and Trios (3Shape, Copenhagen, Denmark) for image acquisition; and CEREC AC (Sirona, Bensheim, Germany) and E4D (D4D Technologies, Richardson, Tex) for digital imaging and in-office manufacturing. Excluding the iTero and the Trios, all scanning devices need drying and powdering of intraoral surfaces (CEREC, E4D, Lava COS). This limits their practicability and accuracy because powder application can add to the measuring error. With all devices mentioned, digital impressions are acquired without contact to the gingival tissues.
The precision of intraoral and extraoral scanning with the iTero as well as extraoral scanning with a model scanner was examined in this study.
Material and methods
Impressions were acquired according to the study protocol that was approved by the ethics committee of the medical faculty of Freiburg University, after we received written consent from the study participant. One participant with a Class I occlusion and full dentition was examined.
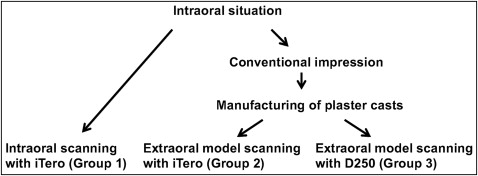
In-vivo (intraoral) scans (group 1) and ex-vivo (extraoral) scans of 1 patient and the patient’s models were made with 2 laser scanners (group 2, iTero; group 3, D250; Fig 1 ).
According to the study protocol, the data acquisition for group 1 was based on 10 intraoral scans with the iTero of the maxilla and the mandible of 1 patient (n = 20).
For groups 2 and 3, a unique model was used. The model fabrication for the extraoral scans was performed as follows.
Using the same patient as in group 1, polyether impressions of the maxilla and the mandible were taken using a monophase polyether material (Impregum Penta; 3M ESPE) and stainless steel impression trays (M+W-Rim-Lock; M+W Dental, Büdingen, Germany). The impressions were disinfected and poured with type IV stone (picodent U 180; Picodent, Wipperfürth, Germany) after a setting time of 4 hours. The first impression was used for the production of the stone casts, independently of the subjective assessment of the quality. One stone cast of the maxilla and 1 stone cast of the mandible were made.
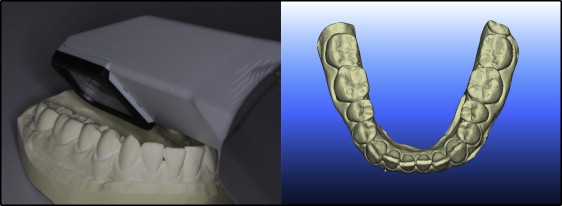
The stone casts were scanned with the iTero using the same scanning protocol as for the intraoral scans. The scans of each stone cast model (maxilla and mandible) were repeated 10 times and produced the data set for group 2 (n = 20).
The virtual models for group 3 (n = 20) were collected by repeated scanning (10 times) of the stone casts with a model scanner (D250).
All scans with the iTero were recorded by the same examiner (T.V.F.) in a predetermined order. Scanning started with the most distal tooth in the third quadrant continuing to the anterior teeth ( Figs 2 and 3 ). Next, the fourth quadrant was scanned, again beginning with the most distal tooth. Scanning of the maxilla started with the most distal tooth in the first quadrant and ended at the central incisor. The second quadrant was recorded starting with the most distal tooth. Each tooth was scanned from its buccal and lingual sides by placing the camera at an angle of 45° to the tooth axis. Images of each tooth showed neighboring parts of adjacent teeth. These served to overlap the pictures to create a model of the whole arch from single images. All models were exported in a Standard Tesselation Language (STL; 3D Systems, Rock Hill, SC) format and were used for evaluation, independently of the subjective assessment.

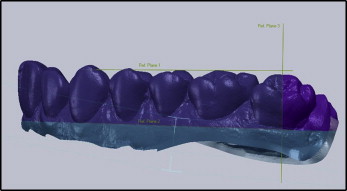
For digitization, the stone casts were placed into the D250 scanner next to a laser source and 2 high-resolution cameras. During the scanning process, the platform moves the model; therefore, the laser reaches the model from multiple angles. Light planes are projected onto the model, and the cameras capture their reflections from the surface ( Fig 4 ).
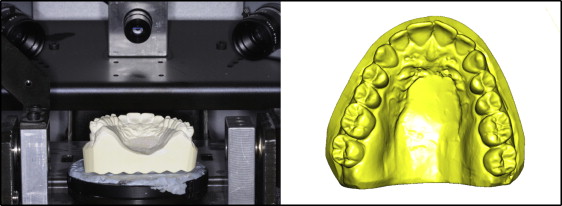
The principle of triangulation was used for the creation of a 3-dimensional model, available as a stereolithographic data set.
All stereolithographic data sets of 1 dental arch and 1 scanning method (n = 10) were imported in a common coordinate system and aligned by a procedure with the closest distance between 2 surfaces (Rapidform XOR; Inus Technologies, Seoul, South Korea). The models were orientated toward the occlusal plane to fit a view for drawing the cutting planes. A first cutting plane running through the deepest point of the gingival sulcus of the canines and the second molars in the maxilla and the canines and the first molars in the mandible was created. A second cutting plane was created running through the transverse fissure of both second molars. All surfaces were cut with the common cutting planes to create equal basal and posterior borders ( Fig 5 ).
For quantitative analysis of precision, deviations between the vertices of the surfaces were measured. Operated scan data were imported into Artec Studio software (version 0.7.3.39; Artec Group, Luxembourg, Luxembourg) to perform a pairwise rigid body registration. Corresponding models for each comparison were roughly aligned manually and then registered onto another using the implemented surface mapping algorithm.
Deviations between aligned models were analyzed using the software package Morpho, version 0.25 (based on R; created by Stefan Schlager, Freiburg, Germany). To estimate the differences between the surfaces, each vertex on the test surface was projected to the closest point on the corresponding control surface, and the Euclidean distance was recorded. The model rendered from the first scan served as the control surface for the consecutively acquired models in each group.
Statistical analysis
Further statistical analysis was performed with the software R. For testing differences between the groups’ distributions of averaged distances, the Kolmogorov-Smirnov test—a distribution free and nonparametric procedure—was applied. The level of significance was set at 0.05.
For the assessment of error, maximum, mean, and median deviations were calculated for each group based on the averaged errors of each observation. The distances between the vertices of the corresponding models were displayed with color maps, so that areas of high and low agreement could be identified.
Results
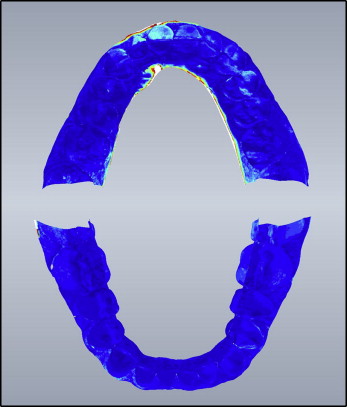
In group 1, the virtual models, rendered from serial intraoral scans of the maxilla and the mandible with the iTero, were compared. The mean deviation was 50 μm (median, 37 μm). Deviations in the maxilla were on average 57 μm (median, 43 μm); the mandible deviated on average 43 μm (median, 31 μm). Maximum deviations were on average 1.137 mm in the maxilla and 717 μm in the mandible. Deviations of the mandible were significantly lower than deviations in the maxilla. Deviations between models are displayed in Figure 6 .
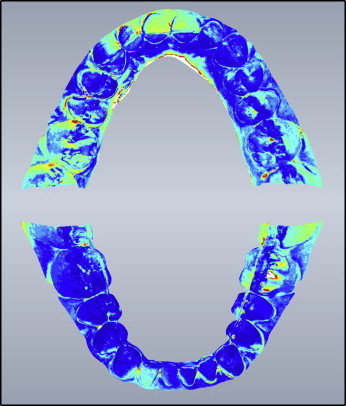
The highest deviations were observed at the palatal borders, the facial surfaces of the anterior teeth, and the molars on both sides of the maxilla. In the mandible, the highest deviations were at the buccal side of the molars and the facial side of the anterior teeth. There were also deviations above average in the interdental spaces.
In group 2, the virtual models acquired with the repeated scans of the stone casts with the iTero were compared. Deviations from the test surface were on average 25 μm (median, 18 μm). The maxillae had a mean deviation of 30 μm (median, 18 μm), whereas the mandibles had a mean deviation of 21 μm (median, 17 μm). The color-coded deviations are depicted in Figure 7 .