Introduction
The increasing success rates for cancer patients treated with radiotherapy and the frequent occurrence of tooth loss during treatment have led to an increased demand for orthodontic treatment after radiotherapy. The aim of this study was to evaluate tooth enamel of irradiated teeth after the bonding and debonding of metal and ceramic brackets.
Methods
Ten permanent molars were cut into enamel fragments measuring 1 mm 2 and divided into an irradiated group (total dose of 60 Gy) and a nonirradiated group. The fragments were subjected to microshear testing to evaluate whether radiotherapy altered the strength of the enamel. Furthermore, 90 prepared premolars were divided into 6 groups and subgroups (n = 15): group 1, nonirradiated and nonaged; group 2, nonirradiated and aged (thermal cycled); group 3, irradiated and aged; each group was divided into 2 subgroups: metallic and ceramic brackets. After thermal cycling and radiotherapy, the brackets were bonded onto the specimens with Transbond XT (3M Unitek, Monrovia, Calif). After 24 hours, the specimens were subjected to the shear tests. Images of the enamel surfaces were classified using the adhesive remnant index. The composite resin-enamel interface was also evaluated.
Results
Enamel fragments subjected to radiation had lower strength than did the nonirradiated samples ( P <0.05). The groups and subgroups submitted to radiation and bonded ceramic brackets had the lowest strength values. Groups 1 and 2 with metallic brackets had less adhesive on the surface, whereas groups 1 and 2 with ceramic brackets and group 3 with both metallic and ceramic brackets had more adhesive on the surfaces. On the images of the composite resin-enamel interface, resin tags were more extensive on irradiated tooth enamel.
Conclusions
Radiation decreased tooth enamel strength, and the specimens treated with radiotherapy had higher frequencies of adhesive failure between the bracket and the composite resin as well as more extensive tags.
Highlights
- •
Irradiated and nonirradiated teeth were bonded and submitted to microshear.
- •
Irradiated enamel showed lower tensile strength when subjected to microshear.
- •
Brackets bonded to irradiated enamel had significant shear strength values.
- •
Irradiated teeth tended to debond at the bracket-composite interface.
- •
Resin tags in the composite-enamel interface were deeper in the irradiated groups.
Each year, approximately 780,000 new cases of head and neck cancer are diagnosed throughout the world, ranking it the fifth most frequent type of cancer. The incidence of cancer tends to be higher as people age. However, studies have shown that the incidence in young people has increased in recent decades. In older patients, the main risk factors are smoking and alcohol consumption, whereas the role of these factors in young patients is uncertain because of the short exposure time. Infection with human papilloma virus is considered a risk factor for this type of tumor and is one possible reason for the increased incidence of head and neck cancer in young patients, since human papilloma virus infections are more frequent in this population and often correlated with sexual behavior.
Radiotherapy is widely used for the treatment of head and neck cancer. It may be recommended as the primary therapy, an adjuvant to surgery and chemotherapy, or a palliative treatment for inoperable cases and the final stages of the disease. Treatment with radiotherapy can have side effects that affect the oral cavity, such as mucositis, xerostomia, diminished sense of taste, trismus, loss of periodontal ligaments, microvascular abnormalities, soft tissue necrosis, osteoradionecrosis, and dental caries. Moreover, studies have demonstrated possible changes in tooth enamel and dentin, such as (1) reduced microhardness, (2) increased microhardness and increased solubility, which reduce stability of the dentinoenamel junction and result in loss of enamel, and (3) atrophy of the odontoblast obliteration process in dentinal tubules. Other consequences of radiotherapy include the loss of structure of enamel prisms, tooth fractures from shearing effects, collagen destruction, an increase of calcium and a reduction in oxygen in the enamel, and breakdown of enamel and dentin, leading to an amorphous surface as well as to cracks and destroyed or collapsed dentinal tubules.
A dental evaluation is needed before cancer treatment. Because of the urgency of beginning radiotherapy, there is often not enough time to perform complex dental procedures. Thus, some teeth end up being extracted because of advanced periodontal disease, extensive dental caries, periapical lesions, and impaction. With the advances in cancer treatment and early diagnosis, cure and survival rates have increased in recent decades. Thus, more dentists are likely to treat patients with a history of cancer treatment.
Orthodontics is a specialty that seeks to establish adequate occlusion as well as to improve chewing ability, function, and esthetics. Orthodontic intervention in patients after radiotherapy should be implemented when the patient has good general health and the risk of the recurrence of cancer has decreased. However, the literature on the optimal period for postradiotherapy orthodontic intervention is sparse. The limited data vary between 1 year and 2 years after the end of radiotherapy.
Corrective orthodontic treatment requires the bonding of brackets to the tooth surface; this can cause structural changes in patients with a history of radiotherapy in the head and neck regions. Although adhesive restorations on irradiated enamel exhibit lower tensile strength and increased susceptibility to cohesive fractures, no studies in the literature have evaluated the bond strength of orthodontic brackets on irradiated teeth.
In patients undergoing radiation therapy, the duration of orthodontic treatment should be short and involve light forces. However, the bonding of orthodontic brackets may be compromised on dental surfaces altered by radiotherapy, leading to a frequent need for rebonding, which extends the length of orthodontic treatment.
The scarcity of information regarding the effects of radiation on the structure of tooth enamel and the absence of studies addressing the adhesion of orthodontic brackets to tooth surfaces justified the need to conduct this study, the aim of which was to evaluate the properties of tooth enamel and the bonding of metal and ceramic brackets on tooth enamel after radiotherapy.
Material and methods
This study received approval from the research ethics committee of the School of Dentistry of the University of São Paulo at Ribeirão Preto in Brazil. Teeth were obtained from the university’s tooth bank.
The sample consisted of 100 sound maxillary and mandibular teeth: a mixture of 10 first, second, and third molars, and a mixture of 90 first and second premolars. Teeth with complete root formation; without dental wear, cracks, fractures, structural abnormalities, or traces of restorations; and no orthodontic, endodontic, or chemical treatment were selected.
The 10 permanent molars were to be subjected to mechanical microshear testing. The root portion of the crown was removed and sectioned to obtain enamel fragments of the buccal and lingual-palatal regions measuring 1 mm 2 . The enamel fragments from each tooth were randomly divided into 2 groups (nonirradiated and irradiated) to have a matched control.
The enamel fragments were embedded vertically in polyvinyl chloride tubes with polyacrylic resin so that 2 mm remained exposed above the resin. The specimens were placed in plastic containers containing artificial saliva and stored at 37°C.
The specimens were irradiated at the Department of Radiotherapy, Clinics Hospital, at the University of São Paulo. During the irradiation procedure, the specimens were placed in plastic boxes and immersed in deionized water to maintain a humid environment simulating the oral cavity. At the end of the procedure, the deionized water was discarded, and the specimens were stored in artificial saliva in a hothouse at 37°C until the next irradiation, when the saliva was again replaced with deionized water. Artificial saliva was not used during irradiation because of the high concentration of ions, which could interfere with the direct radiation per unit of area.
The specimens were submitted to a fractionated dose of 2 Gy over 5 consecutive days for 6 weeks (weekly dose, 60 Gy). The x-rays were emitted from an irradiator devoted to biologic research (RS 2000; Rad Source Technologies, Suwanee, Ga), with energy of 200 kVp and 25 mA and a default copper filter measuring 0.3 mm. X-rays generated under this condition have a spectrum with minimum and maximum energy values of 95 and 200 kV, respectively, and half the value of the beam with 0.62 mm of copper. The gradient of this x-ray dose in tissues is about 10% at a depth of 0.5 cm. Plates were aligned equidistant from the center of the beam and inside the cone to ensure a uniform dose rate (approximately 2.85 Gy/min) and total delivery of the fractionated dose. After radiation, the specimens were kept in artificial saliva at 37°C.
Twenty-four hours after irradiation, the samples were subjected to the microshear test (model 2519-106; Instron, Canton, Mass) with a vertical speed of 0.5 mm per minute using a load cell of 20 kgf.
The premolars (n = 90) were randomly divided into 6 experimental groups ( Table I ) and prepared to undergo the shearing test of the bracket. The dental crown was covered with acrylic resin and polished to achieve a buccal enamel surface area of approximately 5 mm for the bonding of the brackets.
| Group and subgroup | Description |
|---|---|
| Group 1 | Nonirradiated teeth |
| Group 2 | Nonirradiated teeth + aging |
| Group 3 | Irradiated teeth + aging |
| Subgroup M | Metallic brackets |
| Subgroup C | Ceramic brackets |
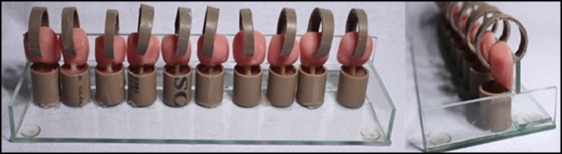
To embed the teeth in the polyvinyl chloride, a device was made from 4-mm glass plates: (1) a base plate, (2) 2 perpendicular plates attached to the sides, (3) a plate fixed horizontally covering half of the base plate, and (4) a perpendicular plate fixed on the side plates. The roots of the teeth were placed centrally in the polyvinyl chloride tubes measuring approximately 1.5 cm in height, which were then filled with self-curing acrylic resin, and the excess resin was removed with a spatula ( Fig 1 ). This device allowed the tooth to remain perpendicular to the base of the tube. This aspect is important to maintain the parallelism between the exposed face of the enamel and the chisel of the shearing during mechanical testing, since any change in angle could affect the result.
Group 3 was subjected to irradiation according to the protocol described above. Two experimental groups (2 and 3) were subjected to accelerated aging with thermal cycling (Biocycle; Biopdi, São Carlos, São Paulo, Brazil) to simulate a period of 1 year, which is suggested in the literature as the minimum time necessary before beginning orthodontic treatment in patients who have had radiotherapy.
Thermal cycling simulates the intake of hot and cold food in the oral cavity by immersing the specimens in water at different temperatures. It is assumed that, in vivo, this cycle occurs 20 to 50 times per day. Thus, the samples were subjected to 10,000 cycles with temperatures between 5°C and 55°C, simulating approximately 1 year. After thermal cycling, the specimens remained in a hothouse at 37°C and were immersed in artificial saliva until the bonding of the orthodontic brackets.
Before bonding, a circular area measuring 5 mm in diameter was established using adhesive tape with a center hole on the buccal surface of the tooth. This area received prophylaxis with extrafine pumice paste and deionized water with a rubber cup at a low speed for 10 seconds, followed by washing for 10 seconds and drying for 10 seconds with a triple syringe free of oil and moisture. Each rubber cup was used on only 5 teeth to prevent the wear of the rubber from affecting the efficacy of the prophylaxis. Acid etching was immediately performed with 37% phosphoric acid for 15 seconds, followed by washing with a vigorous jet of air and water for 10 seconds and drying for 10 seconds.
Next, a thin layer of XT Primer bonding agent (3M Unitek, Monrovia, Calif) was evenly spread over the defined area and light-cured for 10 seconds with an Ultra Blue light-emitting diode unit (DMC USA, Plantation, Fla). The composite resin Transbond XT (3M Unitek) was then applied to the surface of the bracket, which was positioned and pressed with pincers (Orthopli, Philadelphia, Pa) to the vestibular surface. Excess composite resin around the brackets was removed with the blunt tip of an exploratory probe, following by photoactivation. For the metal brackets (Roth standard 18, L12RL; Morelli, Sorocaba, São Paulo, Brazil), light-curing was performed on the mesial, distal, incisal, and cervical faces for 10 seconds on each. For the ceramic brackets (Radiance, L12RL; American Orthodontics, Sheboygan, Wis), light-curing was performed on the mesial and distal faces for 10 seconds each. After 4 photoactivations, the intensity of the light apparatus was measured with a radiometer (Demetron, Danbury, Conn), maintaining an intensity of 600 mW/cm 2 . After bonding the brackets, the specimens were preserved intact for 30 minutes and stored in artificial saliva in a hothouse.
After 24 hours, the samples were subjected to the shear test with the testing machine at a vertical speed of 0.5 mm per minute with a load cell of 20 kgf.
After removing the bracket, the tooth enamel of all samples was evaluated with confocal laser scanning microscopy (LEXT OLS4000; Olympus, Waltham, Mass) and classified based on the adhesive remnant index (ARI), the scoring of which was proposed by Årtun and Bergland : 0, no adhesive left on the enamel; 1, less than half of the adhesive left on the enamel; 2, more than half of the adhesive left on the enamel; 3, all composite resin adhering to the enamel ( Fig 2 ).
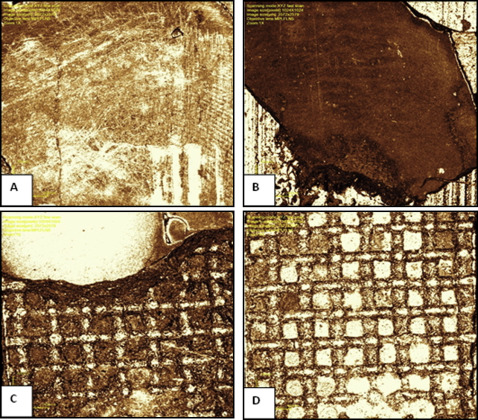
Next, 4 teeth from each group with cohesive fractures were selected, and the crown was cut transversely, dividing the area where the bracket had been bonded. The halves were then subjected to polishing, etching with 37% phosphoric acid for 10 seconds, and washing for 10 seconds. The specimens were dried with a soft tissue and submitted to both laser confocal microscopy and scanning electron microscopy for the examination of the characteristics of the resin tags.
Results
When we analyzed the data, the strength of the dental enamel was significantly decreased by the ionizing radiation (group 1, 11.93 MPa ± 5.62; group 2, 5.96 MPa ± 2.62; P <0.001). In the analysis of the aging factor, group 3 had the lowest adhesion values, differing significantly from the other 2 groups ( P <0.05), whereas no significant difference was found between groups 1 and 2 ( P >0.05). In the comparison of the subgroups (metallic vs ceramic brackets), the mean bond strength was greater when metallic brackets were used ( P <0.05) ( Table II ).
| Group | Subgroups | |
|---|---|---|
| Metallic | Ceramic | |
| G1 | 21.4 ± 3.4 a | 14.9 ± 4.1 b |
| G2 | 21.6 ± 2.9 a | 14.7 ± 3.3 b |
| G3 | 19.1 ± 4.3 a | 10.4 ± 4.2 c |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


