Introduction
The aim of this study was to investigate differences in the periodontal outcomes of palatally displaced canines (PDC) exposed with either an open or a closed surgical technique.
Methods
A multicenter, randomized controlled trial was undertaken in 3 hospitals in the United Kingdom, involving 2 parallel groups. Patients with unilateral PDC were randomly allocated to receive either an open or a closed surgical exposure. Periodontal health was assessed 3 months after removal of fixed appliances. Parameters measured included clinical attachment levels, recession, alveolar bone levels, and clinical crown height.
Results
Data from 62 participants (closed, 29; open, 33) were analyzed. There was no difference between PDC exposed with an open vs a closed surgical technique (mean difference, 0.1 mm; 95% confidence interval [CI], −0.2-0.5). There was, however, a statistical difference in mean attachment loss between the operated and unoperated (contralateral) canines (mean difference, 0.5 mm; 96% CI, 0.4-0.7; P <0.001). Twenty of the 62 subjects had some recession on the palatal aspect of the operated canine, whereas only 4 subjects had some visible root surface on the palatal aspect on the unoperated side ( P = 0.001).
Conclusions
There is a periodontal impact when a unilateral PDC is exposed and aligned. This impact is small and unlikely to have clinical relevance in the short term; however, the long-term significance is unknown. When the open and closed techniques were compared, no difference in periodontal health was found.
Ectopia of the maxillary canine is a common clinical scenario; in orthodontic clinics, its prevalence has been reported to be as high as 13%. Most ectopic canines are palatally displaced, and treatment can be complex, time-consuming, and expensive for both the patient and the health care system. Whereas orthodontic treatment has been found to be mildly detrimental to the periodontium, case reports have described severe periodontal destruction in some cases of aligned palatally displaced canines (PDC).
Burden et al highlighted the controversy in the literature regarding the periodontal outcome of open or closed surgical exposure and subsequent orthodontic alignment of the PDC. Reported periodontal problems included loss of alveolar bone height, increased pocket probing depths, and loss of attached gingivae. Many authors have criticized the open technique because they believe that periodontal health is compromised when the palatal mucosa is excised. This criticism appears to arise from an article published in 1976 about an inherently weak retrospective study of 56 patients with unilateral PDC but was, until now, the only study to directly compare the periodontal consequences of open vs closed surgical exposure. The literature contains less criticism of the closed technique in terms of periodontal impact, although some authors have still reported periodontal concerns when canines aligned with a closed technique are compared with unoperated canines. A recent Cochrane systematic review found no robust evidence to support one surgical technique over the other.
The principal purpose of this trial was to explore any differences in periodontal health between canines exposed with an open vs a closed surgical technique. Differences in periodontal health between canines that had an operation (those that were palatally displaced and had been surgically exposed) vs the contralateral canines that did not have an operation (acting as controls) were also examined.
Two null hypotheses were tested: (1) there is no difference in periodontal health of PDC treated with either an open or a closed surgical exposure, and (2) there is no difference in the periodontal health between operated and unoperated canines.
Material and methods
This was a multicenter, randomized controlled clinical trial involving 2 parallel groups of patients with unilateral PDC, randomized to 1 of 2 surgical exposure techniques and treated in a hospital setting. Ethical approval was obtained from the South Sheffield Ethics Committee (SS02/072) and the North and South Derbyshire local ethics committees (NDLREC ref: 857) in the United Kingdom. Details of our methodology, including the inclusion and exclusion criteria, have been described elsewhere. Once informed consent was obtained from the participants, they were randomly allocated to 1 of 2 interventions. The randomization was undertaken using computer-generated random numbers to ensure that equal numbers were allocated to each intervention; allocation concealment was done with consecutively numbered, sealed, opaque envelopes as outlined previously.
The 2 surgical techniques are summarized briefly below.
For the open surgical exposure, after exposure of the PDC and excision of the palatal mucosa, a surgical pack was sutured in place. After 10 days, the patient was reviewed and the pack removed.
For the closed surgical exposure, after uncovering of the PDC, an eyelet attachment with a gold chain was bonded to the palatal or buccal surface of the ectopic canine (whichever was the most accessible).
Only patients with unilaterally displaced canines were included, so that the contralateral canine could be used as the control.
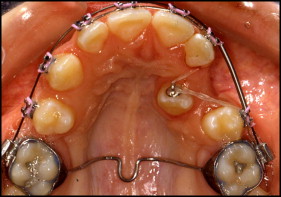
A fixed appliance was placed in the maxillary arch either before or shortly after surgery. For both groups, orthodontic traction was applied using a twin-wire technique or an elastic chain after an 0.018-in stainless steel archwire was in place and there was sufficient space to align the canine. The fundamental difference in orthodontic management was that the canine exposed with the open technique was moved into alignment above the mucosa ( Fig 1 ), and the canine exposed with the closed procedure was moved beneath the mucosa ( Fig 2 ).

Periodontal measurements were recorded at baseline to eliminate the possibility of previous pathology and at 3 months after removal of the fixed appliances. The periodontal outcomes were as follows.
The primary outcome of the trial was the difference in the clinical periodontal attachment level between the PDC treated with the open surgical technique and the PDC treated with the closed technique at 3 months after removal of the orthodontic appliance.
The clinical periodontal attachment level was determined from the 6-point probing depths on the mesial, midline, and distal aspects of the buccal and palatal tooth surfaces, and gingival recession was measured clinically from the visible cementoenamel junction to the gingival margin. The clinical attachment level was calculated as follows: clinical attachment level = periodontal probing depth + gingival recession.
All measurements were made using a Williams Sensor periodontal probe (Hu-Friedy, Chicago, Ill) to the nearest millimeter. This probe is pressure sensitive, and the force is limited to 20 g. The examining clinician was instructed to insert the probe parallel to the long axis of the canine and gently “walk” it around each surface of the tooth.
The secondary outcomes were palatal gingival recession, crown height, and radiographic alveolar bone levels.
Palatal gingival recession was recorded with the following index: (1) cementoenamel junction not visible; (2) cementoenamel junction and less than 2 mm of root surface visible; and (3) cementoenamel junction and 2 mm or more of root surface visible.
The reason for this categorization was the difficulty of clinically measuring recession on the midpalatal aspect of the canine with precision.
Crown height measurements were recorded with calipers to the nearest 0.5 mm from the 3-month postdebond study models.
Alveolar bone levels were measured from periapical radiographs taken between 3 and 12 months posttreatment using computerized image analysis ( Fig 3 ). Although there was some variation as to exactly when the radiographs were taken, the images of the operated and the unoperated sides were obtained at the same time and compared. Film holders (Rinn XCP; Dentsply, Surrey, United Kingdom) and the long-cone technique were used for standardization.
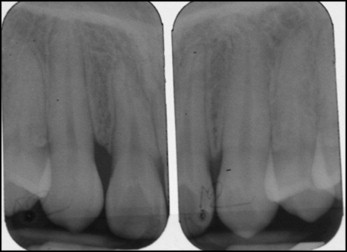
The radiographs were analyzed by quantifying the bone level at the interproximal area between the canine and lateral incisor. This area was chosen because it was the clearest and most consistently imaged site. If not already in digital format, the images were captured with a digital camera (DCS 760; Eastman Kodak, Rochester, NY) suspended above a light box at a standardized distance with standardized shutter speed and aperture settings. Once in digital format, the images were analyzed with computer software (version 7.0, Image-Pro Plus; Media Cybernetics, Rockville, Md) using a technique described previously.
One operator (S.J.B.) made all the measurements on the masked images and repeated them 2 weeks later. The repeatability of the methods was assessed using a paired t test to detect systematic errors and an intraclass correlation coefficient (ICC) to determine random errors. Random errors were low (ICC, 0.896). A potential systematic difference between the first and second readings was detected ( P = 0.034); however, the mean difference between the readings was small (0.09 mm) and considered not clinically significant.
Three clinicians (N.A.P., D.T., A.-M.S.) undertook the direct clinical measurements for the trial. Before their recruitment, training and calibration was undertaken with a specialist restorative dentist (R.S.M.). Percentage agreements ranged from 81% to 88%, with kappa scores of 0.66 to 0.83; these were considered acceptable.
The examiners were masked as to the patient’s group allocation for the clinical examinations. The patient details were removed from all study models and radiographs, which were labeled with only the participant’s randomization number.
An a priori sample size calculation with data from a previous study suggested that for the primary outcome measure of clinical attachment level, a sample size of 60 was required to detect a significant difference between the open and closed exposure groups of 0.5 mm (SD, 0.61 mm; 90% power; 5% significance level; 2-tailed). The sample size was increased to 80 (40 open, 40 closed) to allow for a 25% drop-out rate.
Statistical analysis
Data analysis was divided into 2 sections. The first section compared the 2 surgical techniques; the second section investigated the impact of exposing and aligning a PDC (comparing operated with unoperated canines).
Comparing open versus closed surgical exposure
The difference between the clinical periodontal attachment levels of the operated and unoperated canines in each participant was calculated. Since there was little evidence of any serious deviation from the assumption of normality, independent t tests were used to compare the within-subject mean 6-point clinical periodontal attachment level differences (operated clinical periodontal attachment level minus unoperated clinical periodontal attachment level) between the open and closed groups. To prevent the dilution effect of taking the mean of 6 recordings and also to investigate which areas were most severely affected, the clinical periodontal attachment level at each site was also recorded. The independent samples t test was also used to analyze the data for each site.
For midpalatal and midbuccal recession, the chi-square test for trend was used.
Crown lengths were analyzed by comparing the difference in height between the operated and unoperated canines in the open and closed groups. This relative value assumed that the height of the unoperated canine is the “true” measurement and relates the height of the operated canine to it; this means that variations in actual tooth size will not influence the results. The height of the operated canine was subtracted from the height of the unoperated canine for each participant. The difference was compared using independent samples t tests.
Differences in alveolar bone levels were analyzed by again subtracting the unoperated values from the operated values and comparing the difference between the open and closed groups. Independent samples t tests were used to compare the differences.
Comparing operated versus unoperated canines
Clinical attachment level has been reported as a mean of 6-point probing attachment loss. Because the data were normally distributed, paired t tests were used to compare the differences between the 2 sides. Related Wilcoxon signed rank tests were used to calculate differences between the operated and unoperated canines at each site, since the data were skewed.
The data for palatal recession were categorical, and the McNemar test was used; however, for the midbuccal site, recession was measured to the nearest millimeter, although the maximum value obtained for any subject was only 2 mm. As a consequence, a related Wilcoxon signed rank test was used.
Both crown height and mesial alveolar bone levels were analyzed using a paired samples t test.
Results
Recruitment commenced at the beginning of August 2002 and finished at the end of January 2007. Figure 4 shows the flow of patients through the trial. Eighty-one participants were recruited; however, 10 were excluded from all analyses as outlined in our previous article. Nine participants were excluded from the periodontal analysis: 7 failed to attend follow-up visits (open, 2; closed, 5) and 2, both in the closed group, abandoned treatment midway through the study. Five participants received the incorrect procedure (open, 4; closed, 1); however, the intention-to-treat principle was adhered to, and they were all analyzed in their original allocated groups.
The final sample consisted of 62 participants (open, 33; closed, 29). Details of equivalence between the 2 groups are shown in Table I .
| Open (n = 33) | Closed (n = 29) | |
|---|---|---|
| Age (y) | ||
| Mean (SD) | 14.2 (1.3) | 14.0 (1.6) |
| Sex | ||
| Male | 11 (33%) | 8 (28%) |
| Female | 22 (67%) | 21 (72%) |
| Side of impaction | ||
| Left | 10 (30%) | 13 (45%) |
| Right | 23 (70%) | 16 (55%) |
| Extractions | ||
| Permanent teeth extracted | 13 (40%) | 12 (41%) |
| Duration (mo) | ||
| Duration of active traction | 10.2 (SD, 4.2) | 13.2 (SD, 8.5) |
Comparing open versus closed surgical exposure
The primary outcome of the trial was the mean 6-point clinical periodontal attachment level measurements. When the clinical periodontal attachment level values for the unoperated teeth were subtracted from the clinical periodontal attachment level values for the operated teeth, the mean difference between open and closed groups was just 0.1 mm (open, 0.5 mm, SD, 0.8; closed, 0.6 mm, SD, 0.6); this difference was not statistically significant (independent t test, P = 0.782; Table II ).
| Site | Open (n = 33) | Closed (n = 29) | Differences | ||||
|---|---|---|---|---|---|---|---|
| Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | P value | |
| Mesiobuccal | 0.3 | −0.1-0.8 | 0.8 | 0.3-1.3 | 0.5 | −0.2-1.1 | 0.176 |
| Mesiopalatal | 0.4 | 0.0-0.7 | 0.5 | 0.1-0.9 | 0.12 | −0.4-0.6 | 0.377 |
| Distobuccal | 0.6 | 0.2-1.0 | 0.4 | 0.0-0.8 | −0.2 | −0.8-0.3 | 0.420 |
| Distopalatal | 0.2 | −0.2-0.6 | 0.6 | 0.2-1.0 | 0.4 | −0.1-0.9 | 0.071 |
The mean attachment loss for 3 of 4 sites was found to be marginally greater in the closed group compared with the open group; however, the difference was not statistically significant ( Table III ).
| Side | Mean (mm) | 95% CI | Differences | ||
|---|---|---|---|---|---|
| Mean (mm) | 95% CI | P value | |||
| Open (n = 33) | 1.5 | 1.2-1.8 | 0.1 | −0.2-0.5 | |
| Closed (n = 29) | 1.6 | 1.4-1.9 | |||
| Operated (n = 62) | 1.6 | 1.4-1.7 | 0.5 | 0.4-0.7 | <0.001 |
| Unoperated (n = 62) | 1.1 | 0.9-1.2 | |||
In the midpalate, 8 subjects (28%) in the closed group and 12 subjects (36%) in the open group showed root visibility between 0 and 2 mm. This difference was not statistically significant (chi-square test, P = 0.464).
On the midbuccal aspect of the operated canine, in the closed group, 9 subjects (31%) had recession of at least 1 mm (7 subjects had recession of 1 mm, 2 had recession of 2 mm). In the open group, 8 participants (24%) showed recession of at least 1 mm (5 had 1 mm, 3 had 2 mm). No significant difference was found between the 2 groups (chi-square test, P = 0.774).
The available sample of 66 participants was slightly higher for the outcome measure of crown height (closed, 33; open, 33). The 4 additional patients included in this outcome did not attend their 3-month postdebond recall appointment, but because their immediate debond study models were available, we decided to include them to increase the sample size. These subjects had good oral hygiene and no obvious signs of gingival inflammation or gingival hypertrophy, which, if present, could have affected crown height.
There was considerable variation in the crown lengths between participants (ranges: operated, 6-12 mm; unoperated, 7-12 mm). This necessitated the use of “difference in crown height” between the operated and unoperated canines to compare the open and closed groups (height of operated canine crown minus height of unoperated canine crown). The results are shown in Figure 5 . A positive value indicates that the operated canines had slightly shorter clinical crowns than did the unoperated canines and vice versa. No statistical significance was found between the 2 groups (mean difference, 0.2 mm; 95% CI, −0.29-0.67 mm; independent samples t test, P = 0.43).


