Oral-facial-digital syndrome is characterized by heterogeneous clinical features involving malformations of the face, oral cavity, and digits. The syndrome has been reported only in women, suggesting that it is lethal in males. Affected females have malformations of the oral cavity (cleft palate, lip and tongue, abnormal dentition, and hamartomas), face (hypertelorism and milia), and digits (syndactyly, brachydactyly, and polydactyly). In this article, we report the orthodontic treatment of a 21-year-old woman with oral-facial-digital syndrome.
In 1962, a syndrome characterized by malformation of the face, oral cavity, and digits was reported by Gorlin and Psaume. They called it orofaciodigital dysostosis, a disorder that subsequently was renamed oral-facial-digital syndrome. The prevalence of this syndrome is 1 in 50,000 to 1 in 250,000 live births. Nine oral-facial-digital syndromes have been delineated. Oral-facial-digital syndrome type 1 (OFD1) is the most common type. The other forms are rare; most have been identified in only 1 family or a few families.
The typical clinical characteristics of OFD1 include oral findings affecting primarily the tongue, palate, and teeth. The tongue is lobed and often described as bifid or trifid. Tongue nodules, which are usually hamartomas or lipomas, also occur in at least a third of patients with OFD1. Ankyloglossia attributable to a short lingual frenulum is common. Cleft hard or soft palate, submucous cleft palate, or highly arched palates occur in more than 50% of affected patients. Alveolar clefts and accessory gingival frenulae are common. These fibrous bands are hyperplastic frenulae extending from the buccal mucous membrane to the alveolar ridge, resulting in notching of the alveolar ridges. Dental abnormalities include missing teeth (most common), extra teeth, enamel dysplasia, and malocclusion.
Ocular hypertelorism or telecanthus occurs in at least 33% of affected persons. Hypoplasia of the alae nasi, median cleft lip, or pseudo cleft upper lip are common.
Brachydactyly, syndactyly of varying degrees, and clinodactyly of the fifth finger are common. The other fingers, particularly the third (middle) finger, can show variable radial or ulnar deviation. Duplicated hallux (great toe) occurs in fewer than 50% of affected patients but, if present, is usually unilateral. Preaxial or postaxial polydactyly of the hands occurs in 1% to 2% of affected persons. Radiographs of the hands often show fine reticular radiolucencies, described as irregular mineralization of the bone, with or without spicule formation of the phalanges.
Polycystic kidney disease (unknown frequency) occurs in fewer than 50% of patients. The hair is often described as dry, coarse, and brittle.
Specific findings are observed in oral, facial, and digital structures, which can easily be diagnosed by an orthodontist or a general dentist. Some findings in orthodontic diagnosis and treatment procedures are presented.
Diagnosis and etiology
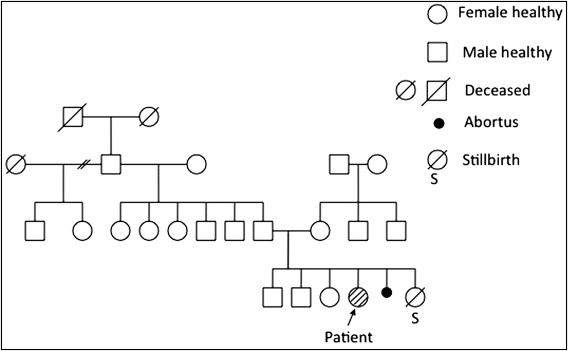
A woman, 21 years 5 months of age, was referred to our orthodontic clinic with chief complaints of misalignment of her anterior teeth and speech problems. A detailed dental, medical, and social history was obtained from the patient. She was a fourth sibling, born to unrelated healthy parents at 30 weeks of gestation. The medical history of the patient’s mother showed an abortion and a stillbirth among her 6 pregnancies. The patient has an older sister and 2 brothers with no congenital anomalies, and no other family members are affected by this syndrome. The pedigree of the patient is shown in Figure 1 .
The clinical examination showed increased exposure of the maxillary incisors with her lips at rest. Her face had a dolichofacial growth pattern with a depressed lower nasal bridge. Posterior rotation of the mandible caused increased lower facial height ( Fig 2 ). When asked, she reported that her hair was dry.

She had Class I right canine and molars, a Class II left canine relationship, an increased overjet, and a unilateral crossbite because of the maxillary transverse deficiency. She had a supernumerary tooth in the mandibular left premolar region. The mandibular right second premolar and left first molar had been previously extracted because of caries ( Figs 3 and 4 ).

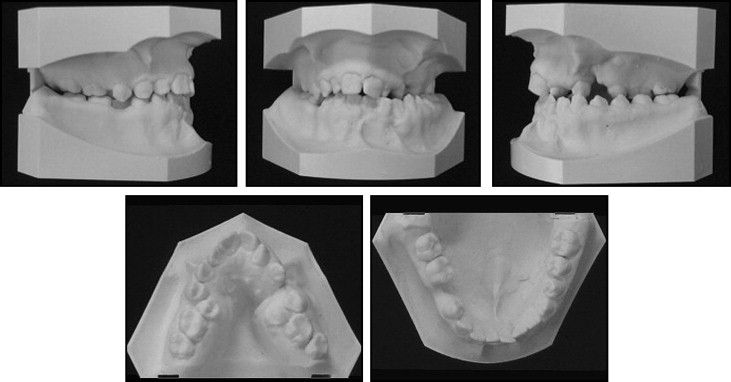
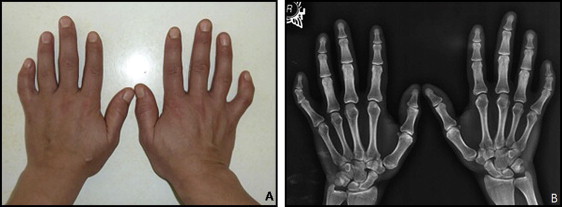
She had the typical findings of OFD1, including bifid tongue, tongue nodules, alveolar cleft in the maxilla, mandibular alveolar notch, and tooth abnormalities ( Fig 5 ). She also had small hands and feet. Brachydactyly and clinodactyly of the fifth finger were determined in both hands, and a radiograph of both feet showed short metatarsals and phalanges ( Figs 6 and 7 ).


A panoramic radiograph showed a supernumerary tooth in the maxillary right premolar region and a root in the right posterior quadrant of the mandible. The lateral cephalogram showed that the mandibular plane angle was steep with an enlarged gonial angle (GoGn-SN, 49°; mean, 32°). The cephalometric analysis showed a mild Class II pattern (ANB, 4.8°; mean, 0°-4°), although the SNA angle of 75.6° (mean, 82° ± 2°) and the SNB angle of 70.9° (mean, 80° ± 2°) showed a retrognathic condition ( Figs 8 and 9 ).



