This article describes the orthodontic treatment of a patient with Lowe syndrome. The objective of the treatment was to improve the patient’s dental relationships and consequently his quality of life. This was achieved by maxillary expansion and extraction of the mandibular central incisors and maxillary deciduous canines. The teeth were aligned and leveled with a fixed orthodontic appliance. Satisfactory results were obtained at the end of treatment, with substantial improvement in dental esthetics, occlusal function, and facial profile.
The oculocerebrorenal (OCRL) syndrome of Lowe, also called Lowe syndrome, is a rare X-linked recessive disorder, distinguished by a triad of organ system abnormalities: ocular disease, such as neonatal-onset cataracts; mental retardation; and renal dysfunction (online Mendelian Inheritance in Man #309000). It was first described by Dr Charles Lowe et al in 1952. It occurs predominantly in white and Asian males. The etiology is related to malfunctioning of the OCRL1 gene on the X-chromosome, resulting in a deficiency of an enzyme called phosphatidylinositol 4,5-biphosphate. The normal activity of the Golgi apparatus, which is regulated by this enzyme, is compromised in patients with Lowe syndrome.
Several reports have described general conditions observed in persons with oculocerebrorenal syndrome. The combination of ocular (neonatal-onset cataracts, glaucoma, and nystagmus), central nervous system (severe psychomotor retardation and hypotonia), and renal (proteinuria, generalized aminoaciduria, and acidosis) manifestations is usually required for identification of this disorder. Other significant common findings include rickets, joint hypermobility, scoliosis, dislocated or subluxed hips, frontal bossing, thin and sparse hair, protruding ears, high-pitched scream, and deviations from the norm in height and weight.
The oral and dental manifestations described in the literature include taurodontism, delayed eruption, enamel hypoplasia, gingival hyperplasia, pericoronal radiolucency, palatal constriction, crowded teeth, vertical facial growth, Class II skeletal malocclusion, underdeveloped mandible, and impacted permanent teeth. The articles available in the literature are concerned only with reporting the clinical manifestations; none address treatment. In an attempt to fulfill this void, the objective of this article was to report the orthodontic treatment of a patient with Lowe syndrome.
Diagnosis and etiology
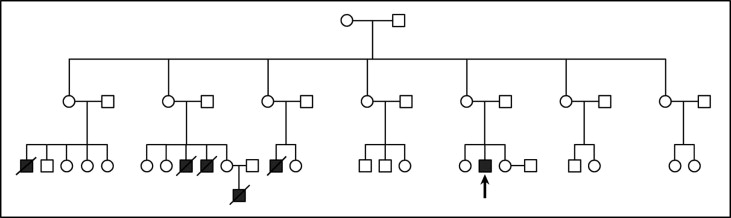
An 18-year-old man diagnosed with Lowe syndrome was referred by his family physician for evaluation of dental problems ( Figs 1 and 2 ). There was a history of Lowe syndrome in the patient’s family ( Fig 3 ). Although his parents and sisters had no medical problems, other relatives had been diagnosed with the condition; they were all deceased before 7 years of age.

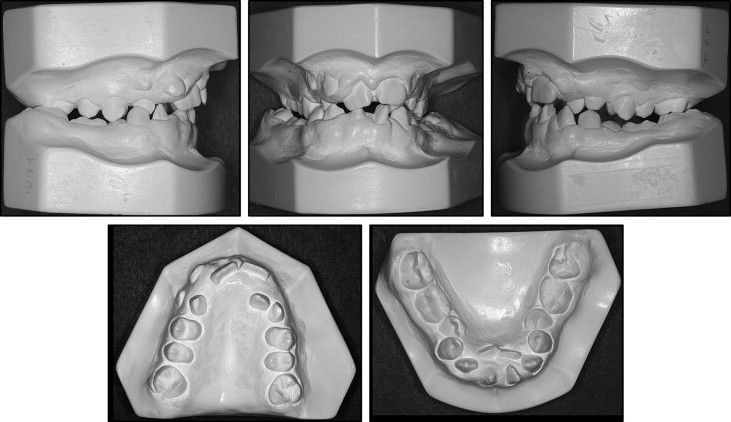
Intraorally, the patient had severe crowding in both arches, gingival hyperplasia, Class III molar relationship, posterior crossbite, lateral crossbite on the right side, constricted maxillary arch, and absence of some teeth. Overjet was normal, and overbite was 3 mm. The extraoral examination showed a remarkably dolichocephalic face with increased lower facial height, frontal bossing, protruding ears, and incompetent lips. He had a severely convex facial profile, a protrusive maxilla, and a retrusive mandible.
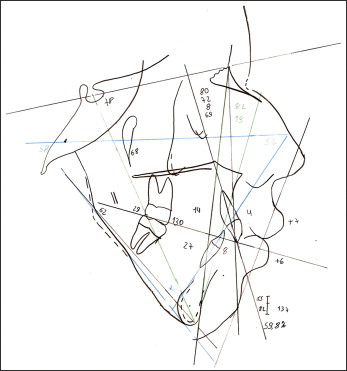
The cephalometric evaluation showed a Class II skeletal malocclusion (ANB, 8°) good maxillary positioning (SNA, 80°), mandibular retrusion (SNB, 72°), vertical facial growth (SnGoGn, 62°; FMA, 58°), retroclined maxillary incisors (1.NA, 14°), and buccally proclined mandibular incisors (1.NB, 27°; 1-B, 8 mm). The facial profile was convex (LS-S, 7 mm; Li-S, 6 mm) ( Fig 4 ).
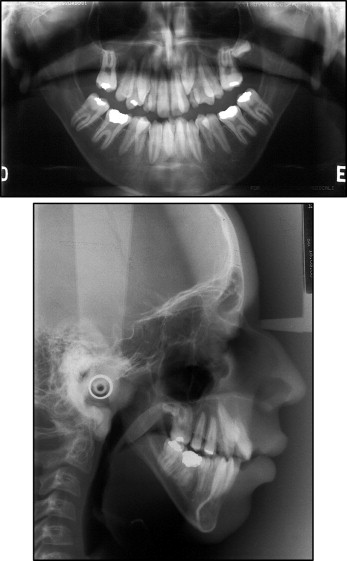
The panoramic radiograph showed taurodontism of the mandibular first molars, retained maxillary deciduous canines, delayed eruption of the maxillary left permanent canine, and delayed development of maxillary left third molar. Ectopic eruption was observed anteriorly in the mandibular arch, probably as a result of the patient’s excessive anterior crowding. In addition, the following teeth were absent: maxillary right third molar, maxillary right first molar, maxillary left first molar, mandibular left third molar, and mandibular right third molar) ( Fig 5 ).
The patient’s oral hygiene was relatively good. His mother showed excellent knowledge of preventive procedures and had carefully helped her son maintain adequate oral health conditions. Nevertheless, he had hyperplasic anterior gingival inflammation in both arches, and hypoplastic enamel was observed in the deciduous canines ( Fig 1 ).
Treatment objectives
The treatment objectives for this patient were to correct the posterior and anterior crossbites, correct the buccolingual inclination of the mandibular posterior teeth, align the teeth and level with traction of the maxillary canines, establish a Class I canine relationship, and achieve normal overbite and overjet.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


