Diagnosis and etiology
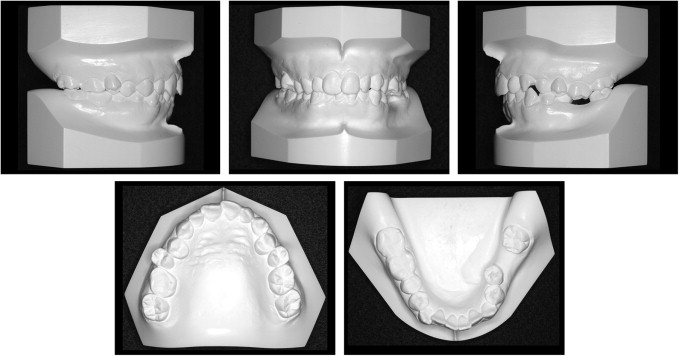
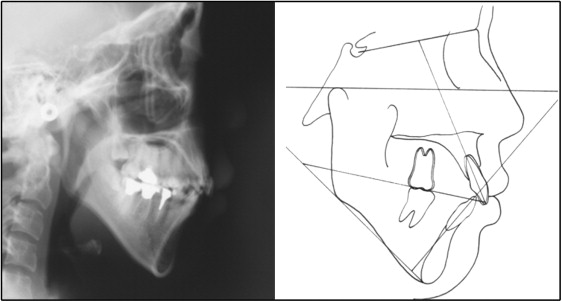
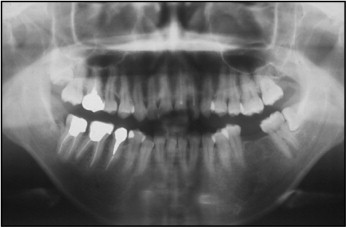
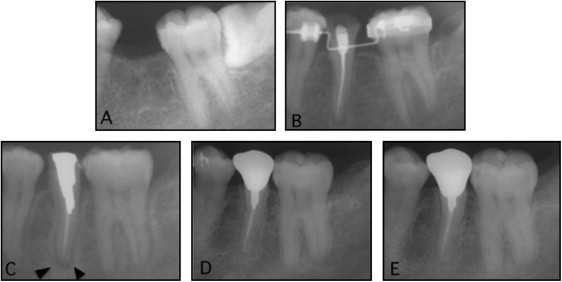
The patient was a Japanese woman, age 29 years 8 months, with chief complaints of maxillary protrusion and absence of the mandibular left first molar, which had been extracted approximately 2 years previously because of severe caries. She had a convex facial profile. Vertically, she had a long face with a high gonial angle. No remarkable facial asymmetry was evident. The intraoral molar relationship on the right side was Angle Class I, and the relationship could not be judged for the left side because of the missing mandibular first molar, although we speculated it to be Angle Class II. The canines exhibited a Class I relationship on the right side and a Class II relationship on the left side. Furthermore, mild maxillary and mandibular crowding was observed. The maxillary dental midline was coincident with the facial midline, and the mandibular dental midline was deviated to the left. The right and left second premolars showed buccal crossbites, and the maxillary left first molar was extruded into the edentulous space of the missing mandibular left first molar. The mandibular left edentulous space measured 7.0 mm; in addition, the mandibular left second molar had a mesial inclination. Overjet and the overbite were 4.0 and 3.5 mm, respectively ( Figs 1 and 2 ). The functional assessment showed no remarkable discrepancy between centric occlusion and centric relation, and no apparent signs or symptoms of temporomandibular disorders. The lateral cephalometric analysis ( Fig 3 , Tables I and II ) showed a skeletal Class II relationship with an ANB angle of 7.0°. Vertically, the patient demonstrated a high-angle tendency (FMA, 44°) and bimaxillary dentoalveolar protrusion (interincisal angle, 117°). Furthermore, a panoramic radiograph showed prior root canal treatment performed for the mandibular right second premolar, first molar, and second molar, and the maxillary right first molar, left central incisor, and lateral incisor. The mandibular left third molar was horizontally impacted with an axial inclination of 90° ( Fig 4 ). No remarkable alveolar bone resorption was observed around the edentulous space of the mandibular left first molar ( Fig 5 , A ).

| Pretreatment | Posttreatment | Postretention | |
|---|---|---|---|
| Angular (°) | |||
| SNA | 79.0 | 79.0 | 79.0 |
| SNB | 72.0 | 72.0 | 72.0 |
| ANB | 7.0 | 7.0 | 7.0 |
| Facial angle | 84.0 | 84.0 | 84.0 |
| Convexity | 15.0 | 15.0 | 15.0 |
| FMA | 44.0 | 44.0 | 44.0 |
| Y-axis | 75.0 | 75.0 | 75.0 |
| Gonial angle | 134.5 | 134.5 | 134.5 |
| Op to FH | 11.0 | 16.0 | 16.0 |
| U1-SN | 101.0 | 90.0 | 91.0 |
| IMPA | 86.0 | 82.0 | 83.0 |
| FMIA | 50.0 | 54.0 | 53.5 |
| Interincisal angle | 117.0 | 132.5 | 130.5 |
| Linear (mm) | |||
| Overjet | 4.0 | 2.0 | 2.0 |
| Overbite | 3.5 | 1.5 | 2.0 |
| Pretreatment | Posttreatment | Postretention | |
|---|---|---|---|
| Maxillary arch width (mm) | |||
| Intercanine | 30.4 | 33.5 | 33.0 |
| Intermolar | 52.7 | 48.6 | 48.7 |
| Mandibular arch width (mm) | |||
| Intercanine | 27.0 | 26.4 | 25.8 |
| Intermolar (second molar) | 51.0 | 50.0 | 52.4 |
Treatment objectives
The primary treatment objectives were as follows: (1) close the edentulous space of the missing mandibular left first molar, (2) establish an attractive facial appearance by retracting the maxillary and mandibular incisors, (3) maintain the vertical facial height without backward rotation of the mandible because of the original long-face tendency, and (4) correct the discrepancy between the facial and dental midlines.
Treatment objectives
The primary treatment objectives were as follows: (1) close the edentulous space of the missing mandibular left first molar, (2) establish an attractive facial appearance by retracting the maxillary and mandibular incisors, (3) maintain the vertical facial height without backward rotation of the mandible because of the original long-face tendency, and (4) correct the discrepancy between the facial and dental midlines.
Treatment alternatives
The treatment alternatives for management of the mandibular left edentulous space were a fixed bridge, dental implants, mesial orthodontic tooth movement of the second and third molars, and tooth transplantation. Even if the treatment for the mandibular left edentulous space failed, it would be necessary to ensure that the posttreatment results were not worse than the pretreatment status. Although a fixed bridge has the advantage of a shorter treatment time, tooth preparation is required for the adjacent teeth. Furthermore, dental implants demonstrate good survival rates but require surgery, and periodontal problems might arise with marginal bone loss around the adjacent teeth and the implants. Mesial orthodontic tooth movement of the second and third molars using miniscrews would not cause the same degree of surgical trauma as that for dental implants or tooth transplantation but has the disadvantage of a longer treatment time.
We therefore planned to extract the bilateral maxillary first premolars, the mandibular right second premolar, and the impacted mandibular left third molar to achieve the treatment objectives. The patient desired tooth transplantation for correction of the mandibular left edentulous space with an extracted tooth as the donor.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


