Introduction
In this study, we examined the impacts of age, sex, root length, bone levels, and bone quality on orthodontic tooth movement.
Methods
Clear aligners were programmed to move 1 central incisor 1 mm over the course of 8 weeks. Thirty subjects, ages 19 to 64, were enrolled, and measurements were made on digital models (percentage of tooth movement goal achieved). Morphometric features and bone quality were assessed with cone-beam computed tomography. Data from this study were combined with data from 2 similar studies to increase the power for some analyses.
Results
The mean percentage of tooth movement goal achieved was 57% overall. Linear regression modeling indicated a cubic relationship between age and tooth movement, with a decreasing rate of movement from ages 18 to 35 years, a slightly increasing rate from ages 35 to 50, and a decreasing rate from ages 50 to 70. The final decreasing trend was not apparent for women. As would be expected, the correlation was significant between the percentage of the goal achieved and the cone-beam computed tomography superimposed linear measures of tooth movement. A significant negative correlation was found between tooth movement and the measurement apex to the center of rotation, but bone quality, as measured by fractal dimension, was not correlated with movement.
Conclusions
The relationship between age and tooth movement is complex and might differ for male and female patients. Limited correlations with cone-beam computed tomography morphology and rate of tooth movement were detected.
The use of clear aligners to produce orthodontic tooth movement (OTM) provides an opportunity to measure incremental movement and investigate factors that might affect the rate of movement. The broad principles of OTM are based largely on bone and tissue remodeling, specifically the resorption and deposition of alveolar bone as force is applied. The biology of OTM has proven to be an extremely complex process involving an array of coordinated biochemical reactions, including critical cell signaling pathways and a wide range of cellular differentiation, leading to bone remodeling. As the science of bone biology continues to evolve, several theories of OTM have surfaced. The pressure-tension theory has emerged as the most popular concept behind the movement of teeth.
Bone remodeling involves an intricate arrangement of coordinated cellular activity leading to bone resorption performed by osteoclasts, followed by bone formation carried out by osteoblasts. Dolce and Holliday have reported that although the precise biologic response to orthodontic force has not been identified, several hypotheses regarding the mechanisms by which osteoblasts and osteocytes sense this initial mechanical stimulus have been proposed, including strain-sensitive ion channels, shear stress receptors, integrin activation, and cytoskeleton reorganization. Three phases of tooth movement have been described in the literature: initial phase, lag phase, and secondary phase. The secondary stage accounts for most of the tooth movement, and teeth during this period move at a faster, more continuous pace.
The magnitude and direction of force placed on teeth during OTM, in addition to the length of time these forces are in place, also play critical roles in how teeth move. Forces applied to teeth cause various types of tooth movement depending on the location of the center of resistance of that tooth and the direction in which the force is applied. It is understood that the center of resistance for a given tooth changes based on tooth size, number of roots, and amount of tooth root that is submerged in bone.
Variability among patients can affect OTM. Factors including age, sex, root length, bone levels, bone density, medications, and certain systemic conditions can have inhibitory, synergistic, or additive effects on OTM. The majority of literature on the effects of age on OTM has been completed using animal models. Bridges et al reported that a significantly greater amount and rate of tooth movement occurred in younger rats compared with their older counterparts in all 3 phases of tooth movement. Similar findings of the effects of increasing age on the rate and amount of tooth movement have been reported by Misawa-Kageyama et al and Harris. There has also been some indication that whereas there is a delay in the onset of tooth movement in adult rats, once the secondary phase of tooth movement is reached, the movement becomes equally efficient among the 2 age groups. The effect of age on OTM clearly exists and is likely due in part to a decreased biologic response. Although there is individual variability from patient to patient, a direct difference in OTM between the sexes has not been shown in the literature.
Medications with pharmacologic effects can impact the cells targeted in OTM. Some of these medication classes include bisphosphonates, estrogens, NSAIDS and other analgesics, corticosteroids, calcium regulators, and supplements. There is little human experimental data on the effects of medications on OTM and limited information from animal models. However, knowing the biochemical action of these medications has led to concerns regarding how they can affect orthodontic treatment. Any medication that interferes with or alters bone biology might impact the rate of tooth movement.
Systemic factors or nutritional deficiencies affecting bone metabolism have also been found to alter OTM. Specifically, diseases of bone can have a significant impact on the rate of tooth movement as well. Reduced or complete lack of osteoclast function can lead to a condition known as osteopetrosis, characterized by sclerosis of the skeleton and inhibited tooth movement and eruption. On the other hand, in Paget’s disease, uncontrollable bone turnover occurs because of the overactivity of osteoclasts. Since OTM stimulates an inflammatory process in the periodontal ligament and surrounding tissues, it is thought that any chronic inflammatory disease such as thyroiditis, asthma, and even allergies can affect the movement of teeth.
Other variables that might be of significance in OTM are root length, bone levels, and the density or quality of bone. Age-related decreases in bone turnover as well as a relatively higher level of bone density have been documented. Alveolar bone levels, on average, decrease over time, impacting OTM by changing the center of resistance. The center of resistance of a tooth is largely influenced by its surroundings, particularly in regard to root morphology, bone levels, and bone quality. Thus, patients with alveolar bone loss or abnormally long roots will have centers of resistance farther from the point of force application (more apically). Alternatively, the more the root tapers, the more the center of resistance moves coronally.
Clear aligners with sequentially programmed movement provide an excellent model for investigating tooth movement. A single tooth can be isolated, and frequent measurements made with polyvinyl siloxane or digital impressions provide incremental information regarding the pattern of movement. For example, McGorray et al characterized the weekly pattern of tooth movement using this model over 8 weeks, along with subsequent relapse. Kravitz et al compared actual tooth movement with aligners with predicted movement over the course of treatment. Aligner treatment is now a commonly prescribed modality for OTM in adolescents and adults, and a better understanding of the pattern of movement and factors that influence movement could lead to more efficient treatment.
The purposes of this study were to better characterize the pattern of tooth movement with clear aligners with programmed movement over 8 weeks and to examine the influence of age, sex, root length, morphometric measurements, and bone quality on the rate of OTM.
Material and methods
The design for this study was similar to 2 previous studies that investigated specific aspects of tooth movement with clear aligners. Approval was obtained from the University of Florida Institutional Review Board for the Protection of Human Subjects. This project was a prospective single-center clinical trial involving subjects of 2 age groups with minor incisor malalignments, who were otherwise healthy and would be undergoing orthodontic treatment. The first group included 7 men and 8 women between the ages of 18 and 35 years, inclusive. The second group consisted of 5 men and 10 women 50 years of age and older. Throughout this article, this study will be called Study 3. Study 1 investigated the role of relaxin in tooth movement and relapse, and has been previously described. No difference in tooth movement was detected when comparing those who received relaxin injections with those who received placebo injections; thus, data from both groups in this study were combined, yielding a sample size of 37 subjects. Cone-beam computed tomography (CBCT) imaging was not performed in Study 1. Study 2 was similarly designed but included CBCT imaging and examined the role of aligner material fatigue in tooth movement. Subjects in this study received a new aligner every week rather than every 2 weeks as in Study 1. No difference was detected in total tooth movement when comparing the weekly aligner and the biweekly aligner groups. For studies 1 and 2, the biweekly tooth movement goal was 0.50 mm, for a total 8-week goal of 2 mm. Study 3 was designed to broaden the age range and to be used in conjunction with the previous studies to examine the role of age and other factors in tooth movement. In the 3 studies combined, the total number of subjects was 82. All subjects were in good health and had acceptable malocclusions as defined in the inclusion criteria, which have been described in a previous study.
Once a subject was accepted into the trial, the right or left maxillary central incisor was selected as the target tooth. The selection was based on the target tooth’s not being blocked out by the adjacent teeth to allow a total anteroposterior movement of 1 mm. Tooth movement was accomplished using a series of 4 maxillary aligners (Invisalign; Align Technology, San Jose, Calif), each programmed in increments of 0.25 mm of anterior movement of the central incisor being studied, as described above. Aligners were collected every 2 weeks from each subject, and new aligners were dispensed. The study termination visit and final time point for data collection was at week 8. Polyvinyl siloxane impressions were taken weekly and sent to Align Technology for scanning to create 3-dimensional models. Tooth movement measurements from baseline through week 8 were made from each scanned model using ToothMeasure proprietary software (Align Technology). CBCT measurements and fractal analysis were completed using a combination of software including InVivo (Anatomage, San Jose, Calif), ImageJ (National Institutes of Health, Bethesda, MD), and Tact Workbench (Wake Forest University, Winston-Salem, NC).
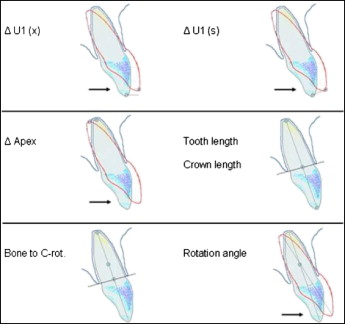
The following are definitions of the measurements used in the CBCT superimposition analysis. Δ U1 (x) refers to the distance between lines drawn through the midpoint of the incisal edges of the superimposed target tooth perpendicular to the anteroposterior axis (the plane of prescribed tooth movement). Δ U1 (s) is the length of the line connecting the midpoint of the incisal edges of the superimposed target tooth. Δ Apex refers to the length of a line connecting the change in apex of the superimposed target tooth. Rotation angle is the angle created by the intersection of lines drawn from the midpoint of the incisal edge to the apex of the target tooth. The apex of this angle is considered the center of rotation. Tooth length refers to the distance from the midpoint of the incisal edge to the apex of the target tooth from the initial computed tomography image. Crown length is the portion of the tooth length that is coronal to the bone. Bone to C-rot is the section of tooth length between the center of rotation and a line connecting the most coronal aspect of the faciolingual crestal bone. These variables are illustrated in Figure 1 .
All study subjects were instructed to wear the aligner appliance full time. They were allowed to remove the appliance when eating, drinking, or brushing their teeth. Their medication and medical histories were taken initially. Each subject recorded aligner wear time in a diary format. At the conclusion of the study, the participants were routinely treated orthodontically with clear aligners.
To determine subject eligibility, 2 visits were required. The first visit was designed to identify potential subjects with malocclusions needing minor incisor alignment of at least the maxillary incisors. Those with medical conditions or intraoral problems, including significant periodontal disease, chronic daily use of any nonsteroidal or anti-inflammatory medication, current smokers, or history of significant cardiac disease, uncontrolled hypertension, bleeding disorders, or renal disease, were also excluded. Subjects who were determined to be eligible based on these procedures proceeded to the next visit.
The screening visit was designed to finalize the subject’s eligibility and collect initial records. The following procedures were performed at this visit: impressions were taken with polyvinyl siloxane for preparation of the Invisalign appliances, impressions were sent to Align Technology after confirmation of eligibility, and intraoral and extraoral photographs and CBCT imaging were done. For women, a negative urine pregnancy test immediately before this procedure was required. After the investigator (T.T.W.) reviewed all subject information to confirm eligibility, the subjects were enrolled into the study and assigned a unique number.
At the first study visit (week 0), the first aligner was delivered to each subject. The acceptable visit window for weeks 1 through 8 was ± 1 day, and all 30 treatment subjects successfully satisfied this requirement.
During the study visits of weeks 1 through 8, the following procedures were performed: intraoral clinical examination, maxillary occlusal and frontal photographs, and polyvinyl siloxane impressions. In addition, during the study visits of weeks 2, 4, and 6, the aligner (used during the previous 2 weeks) and the wear diary were collected, and the next aligner and diary were dispensed. At the study termination visit, week 8, the same procedures were performed, and CBCT imaging of the maxilla took place.
Weekly anteroposterior movement of the target tooth was recorded with polyvinyl siloxane impressions. These impressions were sent to Align Technology, and digital models were created so that OTM could be measured using Align Technology’s ToothMeasure software. The digitized model fabricated each week was superimposed on the baseline digital model, taken at week 0, according to the best fit of unmoved teeth, particularly the posterior dentition. The most central portion on the facial surface of the clinical crown of the target tooth, referred to as the centroid, was determined, and subsequent tooth movements in all dimensions were measured from this point at each study visit. The same investigator (J.R.C.) measured the digital models for all 30 subjects.
CBCT scans of each subject were performed at the screening visit and at the study termination visit (week 8). Using the InVivo software, the images were superimposed on each other and registered at the curvature of the palate in addition to other stable maxillary structures. Measurements recorded from these superimpositions are shown in Figure 1 . A fractal dimension score was calculated for each subject, representing the quality of the bone. Higher fractal dimensions correspond to greater morphologic complexity of the bone.
Weekly wear time was calculated for each subject, with mean, median, and standard deviation of weekly wear time used to characterize each participant’s wear patterns.
Statistical analysis
Orthodontic tooth movement was quantified using descriptive statistics for the digital model analysis. Chi-square tests of equality of proportions and analysis of variance (ANOVA) were used to compare subject characteristics and results over the 3 studies. To standardize the studies, the primary outcome was the percentage of tooth movement goal achieved over 8 weeks. Spearman correlation coefficients were estimated to examine the relationship between that outcome variable and age, morphometric measurements, and compliance. Median weekly hours of wear were used to represent compliance during the study, and this would not be overly influenced by a week of limited wear or excessive wear and would better represent typical weekly compliance. Linear regression modeling was used to examine the relationship between the percentage of tooth movement goal achieved and multiple covariates. Based on the R 2 value (percentage of variability in the outcome explained by the model), the best 1, 2, 3, and so on variable models were determined. Model building was concluded when additional variables did not significantly improve the previous model. Potential interactions between covariates and the influence of outliers were also examined. A P value less than 0.05 was considered statistically significant, and analyses were performed using SAS software (version 9.1.3; SAS Institute, Cary, NC) and R software (version 2.15; R Foundation for Statistical Computing, Vienna, Austria).
Results
The demographic characteristics of the subjects for the 3 studies can be found in Table I . No significant differences were detected when comparing the studies for sex, race, compliance, and percentage of tooth movement goal achieved. Tooth movement goal and age were not compared because they differed in the designs of the studies. The pattern of tooth movement over 8 weeks is shown in Figure 2 . Most tooth movement occurred in the first week of the 2-week wear cycle.
| Study 1 (n = 37) | Study 2 (n = 15) | Study 3 (n = 30) | Total (n = 82) | P value | |
|---|---|---|---|---|---|
| Sex, female (%) | 70 | 60 | 60 | 65 | 0.63 ∗ |
| Race (%) | |||||
| White | 76 | 54 | 77 | 72 | 0.32 ∗ |
| Black | 13 | 13 | 10 | 12 | |
| Other | 11 | 33 | 13 | 16 | |
| Tooth movement 2-week goal | † | ||||
| 0.25 mm (%) | 0 | 0 | 100 | 37 | |
| 0.50 mm (%) | 100 | 100 | 0 | 64 | |
| Age (y), median | 27.1 | 23.1 | 43.5 | 27.9 | † |
| Mean (SD) | 26.7 (5.1) | 25.1 (4.9) | 40.7 (15.5) | 31.5 (12.3) | |
| Range | 18.6-40.5 | 20.0-35.0 | 19.0-68.0 | 18.6-68.0 | |
| Compliance, median hours/wk | (n = 34) | (n = 15) | (n = 30) | (n = 79) | 0.13 ‡ |
| Mean (SD) | 138 (24) | 144 (14) | 147 (8) | 142 (18) | |
| Range | 28-162 | 104-157 | 128-160 | 27-162 | |
| % goal achieved, median | 59.0 | 58.0 | 68.0 | 61.8 | 0.17 ‡ |
| Mean (SD) | 53.2 (16.2) | 55.4 (15.0) | 61.6 (20.0) | 56.9 (17.7) | |
| Range | 11.0-77.5 | 17.5-73.0 | 11.0-93.0 | 11.0-93.0 | |
∗ Chi-square test of equality of proportions.
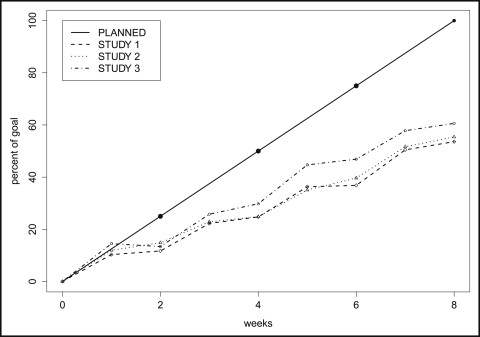
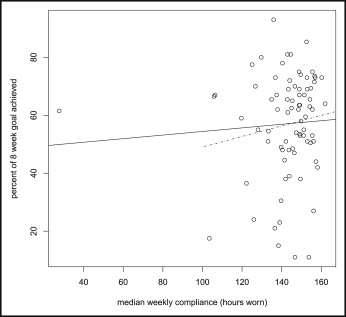
Table II presents summary statistics and group comparisons for the demographic variables and planned biweekly tooth movement. The percentage of the goal achieved did not differ significantly by sex or race. Although it was not statistically significant ( P = 0.06), subjects with a smaller goal had a higher mean percentage of goal achieved, 62%, compared with 54% for those with a planned movement of .50 mm. There was no significant correlation with age, according to the Pearson correlation coefficient estimate of −0.021 ( P = 0.90). However, examining this correlation separately for men and women, different patterns were suggested, with the women having a positive correlation coefficient estimate, 0.09 ( P = 0.52), whereas the men had a negative correlation coefficient estimate, −0.23 ( P = 0.25). We also did not detect a significant correlation between compliance (measured by median weekly hours worn) and percentage of goal achieved, with the Pearson correlation coefficient estimate of 0.06 ( P = 0.59). This relationship is displayed in Figure 3 .
| Variable | n | Mean | SD | Range | P value ∗ |
|---|---|---|---|---|---|
| Sex | |||||
| Male | 29 | 54.4 | 16.1 | 17.5-80.0 | 0.35 |
| Female | 53 | 58.2 | 18.5 | 11.0-93.0 | |
| Race | |||||
| White | 59 | 58.0 | 16.1 | 11.0-93.0 | 0.37 |
| Black | 10 | 58.4 | 19.4 | 24.0-85.3 | |
| Other | 13 | 50.5 | 22.8 | 15.0-77.5 | |
| Goal | |||||
| 0.25 mm | 30 | 61.6 | 20.0 | 11.0-93.0 | 0.06 |
| 0.50 mm | 52 | 54.1 | 15.8 | 11.0-77.5 |
Summary statistics for the CBCT measurements and their correlations with percentage of goal achieved are given in Table III . High correlation would be expected between percentage of goal achieved and ΔU1(x), ΔU1(s), and rotation angle, since these should correspond well with the model-based tooth movement percentage of goal achieved measurement. Significant correlations were not noted for most morphometric measures. A negative correlation with percentage of goal achieved was identified for the apex to center of rotation measurement; this is illustrated in Figure 4 .


