To reduce a large amount of mandibular setback and to prevent pharyngeal airway space narrowing when correcting a severe anteroposterior skeletal discrepancy, a mandibular step osteotomy is often combined with 2-stage orthognathic surgery. This case report describes a successful 2-stage orthognathic treatment combined with a mandibular step osteotomy. A 20-year-old man had severe mandibular protrusion, facial asymmetry, and macroglossia. Phase 1 surgery included the mandibular step osteotomy and a partial glossectomy; then we performed phase 2 surgery with a 2-piece LeFort I segmental osteotomy and a bilateral intraoral vertical ramus osteotomy to correct the patient’s mandibular protrusion and facial asymmetry. The total treatment period was 30 months, and the final result was improvement of the patient’s facial appearance.
A combination of orthodontic treatment and orthognathic surgery is often used for adult patients with excessive anteroposterior skeletal Class III discrepancies. Several methods have been described for the surgical correction of mandibular prognathism. However, there are some limitations of orthognathic surgery for Class III malocclusions related to the possibility of postsurgical relapse. Common factors accounting for surgical relapse are the amount of mandibular setback and stretching of the pterygomasseteric sling, which is related to the forward muscular pull. In addition, a large amount of mandibular setback might lead to pharyngeal airway narrowing, causing obstructive sleep-related breathing disorders.
To reduce a large amount of mandibular setback when correcting a severe anteroposterior skeletal discrepancy, a mandibular step osteotomy is often used in combination with a 2-jaw surgery. A mandibular step osteotomy reduces the mandibular body length and a large overjet by closure of bilateral preexisting edentulous spaces or by extraction of 2 teeth; in addition, it might correct crossbites in the buccal segments by tilting the posterior fragment lingually. This case report describes a successful 2-stage orthognathic treatment that included a mandibular step osteotomy in a patient with an excessive anteroposterior skeletal Class III discrepancy, facial asymmetry, and macroglossia.
Diagnosis and etiology
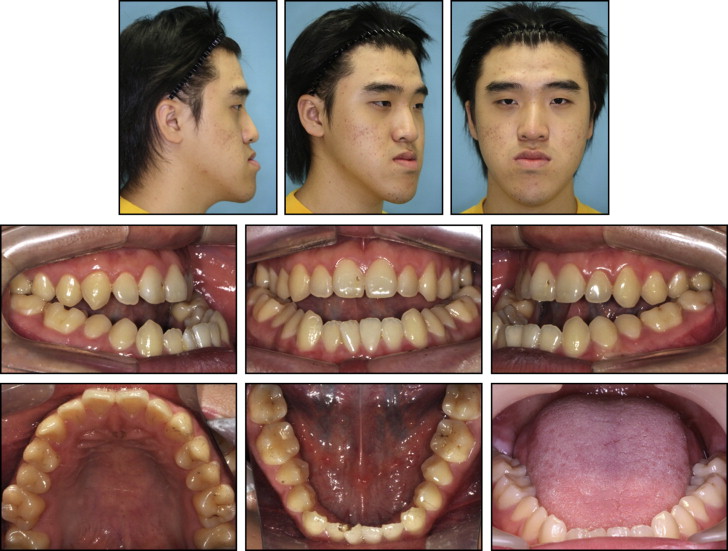
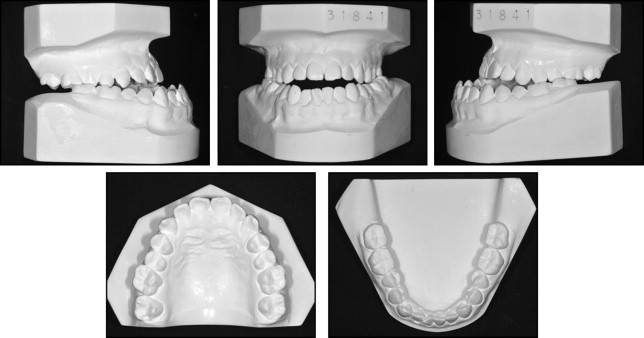
A 20-year-old man visited the orthodontic department at Yonsei University Dental Hospital in Seoul, Korea, with chief complaints of mandibular prognathism and anterior crossbite. On the pretreatment questionnaire, he reported a strong desire to improve his facial appearance. He had no serious medical history but had a clicking sound from the left temporomandibular joint. Pretreatment facial photographs showed a mandibular deviation toward the right and a paranasal depression. His mouth corners were at noticeably different levels. Maxillary incisor exposure was 0.0 mm at rest ( Figs 1-3 ). Intraorally, he had an Angle Class III malocclusion on both sides and macroglossia. Overjet and overbite were −12.0 and −5.0 mm, respectively. The maxillary dental midline showed a 1.5-mm deviation toward the right, and the mandibular dental midline had a 3.5-mm deviation toward the right. The maxillary arch form was relatively constricted compared with the mandibular arch form. He had relative macroglossia with bite marks on the bilateral sides of the tongue. There was little space in the oral cavity when the tongue functioned. A lateral cephalometric analysis showed an SNA angle of 82.0°, an SNB angle of 89.2°, and an ANB angle of −7.2°. The mandibular plane angle was 39.9°, and the gonial angle was large, at 137.1°. The mandibular body length was 95.0 mm. The mandibular incisors were inclined lingually, at an angle of 70.1° toward the mandibular plane. The upper lip was retrusive, and the lower lip was protrusive with respect to the esthetic E-line. The posteroanterior cephalometric analysis indicated that the maxillary molars extruded 1.0 mm more on the left side than on the right side, and the mandibular chin top was deviated 3.5 mm toward the right. The panoramic and periapical radiographs showed a supernumerary tooth between the maxillary central incisors. Two third molars in the mandible were impacted, and the periodontal tissues were healthy ( Figs 1 and 3 , Table ).

| Measurement | Norm | Pretreatment | Postphase 1 surgery | Posttreatment |
|---|---|---|---|---|
| Skeletal | ||||
| SNA (°) | 82.4 ± 3.2 | 82.0 | 81.5 | 82.1 |
| SNB (°) | 80.4 ± 3.1 | 89.2 | 85.4 | 77.7 |
| ANB (°) | 2.0 ± 1.7 | −7.2 | −3.9 | 4.4 |
| Wits (mm) | −2.0 ± 2.4 | −29.8 | −18.8 | −12.4 |
| SN-GoGn (°) | 32.0 ± 5.0 | 39.9 | 43.7 | 54.2 |
| Gonial angle (°) | 117.1 ± 6.7 | 137.1 | 140.3 | 142.3 |
| Go-Me (mm) | 79.0 ± 5.0 | 95.0 | 87.4 | 82.7 |
| Dental | ||||
| U1 to SN (°) | 107.0 ± 5.0 | 108.2 | 108.8 | 95.7 |
| L1 to GoGn (°) | 95.0 ± 5.0 | 70.1 | 77.1 | 78.6 |
| Soft tissue | ||||
| Upper lip E-line (mm) | 1.0 ± 2.0 | −4.6 | −1.6 | 0.1 |
| Lower lip E-line (mm) | 2.0 ± 3.0 | 4.6 | 4.6 | 2.8 |
Treatment objectives
Based on the cephalometric findings, this patient was diagnosed with a skeletal Class III malocclusion with mandibular protrusion, facial asymmetry, and macroglossia. The following treatment objectives were planned: (1) correct the patient’s facial asymmetry and coordinate the facial, maxillary, and mandibular dental midlines; (2) correct the skeletal Class III anteroposterior jaw relationship; (3) coordinate the widths of the dental arches; (4) correct the canted occlusal plane and achieve an ideal overjet and overbite relationship; (5) relieve dental compensation by straightening the mandibular incisors to an upright position over the basal bone; (6) shorten the tongue to prevent postoperative recurrence; and (7) extract the impacted supernumerary tooth.
Treatment objectives
Based on the cephalometric findings, this patient was diagnosed with a skeletal Class III malocclusion with mandibular protrusion, facial asymmetry, and macroglossia. The following treatment objectives were planned: (1) correct the patient’s facial asymmetry and coordinate the facial, maxillary, and mandibular dental midlines; (2) correct the skeletal Class III anteroposterior jaw relationship; (3) coordinate the widths of the dental arches; (4) correct the canted occlusal plane and achieve an ideal overjet and overbite relationship; (5) relieve dental compensation by straightening the mandibular incisors to an upright position over the basal bone; (6) shorten the tongue to prevent postoperative recurrence; and (7) extract the impacted supernumerary tooth.
Treatment alternatives
The following treatment alternatives were considered based on the objectives: (1) 1-stage maxillary and mandibular orthognathic surgery with clockwise rotation, without 2-piece segmental surgery; and (2) 2-stage maxillary and mandibular orthognathic surgery: phase 1 surgery would include the mandibular step osteotomy with extraction of the first 2 premolars, and phase 2 surgery would include maxillary and mandibular orthognathic surgery with clockwise rotation and 2-piece maxillary segmental surgery. Both options included extraction of the impacted mesiodens and a partial glossectomy. The advantages of option 1 were the short treatment duration, no need for maxillary segmental surgery and the extraction of mandibular first premolars, and establishment of a dental Class I canine-molar relationship. However, the surgical treatment objective required a large amount of mandibular setback (20.0 mm), stretching of the pterygomandibular sling, and narrowing of the pharyngeal airway ( Fig 4 , A ). On the other hand, the disadvantages of option 2 included a long treatment duration, a maxillary segmental osteotomy, and establishment of a Class III molar relationship after extraction of 2 teeth. However, the mandibular setback and stretching of the pterygomandibular sling would be decreased when the mandibular body length was reduced ( Fig 4 , B ). The patient agreed to a 2-stage orthognathic treatment.


